
The complex role of RhoA in regulating vascular smooth muscle cell phenotype in Type 2 diabetes
 0
0
Abstract
The incidence of type 2 diabetes mellitus (T2DM) is growing globally, and the major cause of morbidity and mortality in these patients is the premature development of cardiovascular disease. Consequently, medical interventions, such as coronary artery bypass graft surgery and widespread statin prescriptions, are common in this patient group. Smooth muscle cells are the major structural component of the vascular wall. They play a crucial role in post-bypass recovery to successfully revascularize the heart by switching between differentiated (contractile) and dedifferentiated (synthetic) phenotypes. However, in patients with T2DM, these cells have functional defects that may affect bypass integration. RhoA is a small GTPase that regulates many functions, such as motility and phenotypic regulation of smooth muscle cells. RhoA is dependent upon a stimulus, and it can drive the contractile smooth muscle cell phenotype present in the healthy condition or the (mal)adaptive phenotypes prevalent in disease or in response to injury. We hypothesize that RhoA deregulation plays a major role in vascular complications of T2DM. This protein is deregulated in T2DM smooth muscle cells, which may in part explain the functional defects of smooth muscle tissue and the subsequent failure rate of bypass in these patients. An important consideration in this circumstance is the use of statin therapies because these further inhibit RhoA activity. The effect of inhibition of RhoA activity in patients with T2DM who have a bypass is currently unknown.
Keywords
INTRODUCTION
The incidence of type 2 diabetes mellitus (T2DM) is escalating at an alarming rate, and 7% of people worldwide are expected to suffer from T2DM within the next decade[1]. The leading cause of morbidity and mortality in these patients is the premature development of microvascular and macrovascular complications, such as extensive atherosclerotic lesions leading to heart attacks, stroke and peripheral artery disease[2]. Smooth muscle cells (SMCs) are the principal cell type in the vascular wall. Therefore, understanding how these cells behave and respond to challenges in T2DM is critical for the development of new therapeutic avenues that are required to address this global crisis. This review article examines the hypothesis that RhoA is an attractive target for improving vascular health in diabetes through its actions in SMCs.
SMCs are contractile and have inherent plasticity and ability to dedifferentiate into a number of phenotypes to maintain vessel function following a challenge. This is an important adaptation in response to injury, disease or age. However, this adaptation can quickly become maladaptive if the exquisite sensitivity to phenotypic cues is lost[3]. The molecular pathways controlling the SMC phenotype are well recognized. The serum-response factor (SRF) - myocardin signaling axis is a major determinant of SMC differentiation. Under normal healthy conditions, myocardin and myocardin-related transcription factors (MRTF-A and MRTF-B) are shuttled from the cytoplasm into the nucleus where they associate with SRF. Once combined, these complexes bind as transcription factors to areas of the genome containing CArG cis elements (CC(A/T)6GG). This binding increases the expression of classical contractile SMC markers, such as alpha smooth muscle actin (α-SMA; ACTA2), smooth muscle myosin heavy chain, smooth muscle 22 alpha, calponin and smoothelin[4]. These proteins play structural roles in SMC contraction and maintain vessel homeostasis.
In aging, repair or disease, SMCs transiently adopt a synthetic phenotype. External cues, such as platelet-derived growth factor-BB (PDGF-BB), upregulate Kruppel-like factor 4 (KLF4) expression. This protein has an inverse relationship with myocardin and, when expressed at high levels, inhibits myocardin, which is no longer available as a co-factor for SRF. Therefore, the expression of contractile machinery falls. KLF4 also upregulates pro-inflammatory nuclear factor kappa B (NFκB) signaling and SMC dedifferentiation[5]. However, there is no definitive “SMC” phenotype. The SMC phenotype exists along a spectrum from contractile to synthetic, and is fluid regarding protein expression and ion channel types across different vessels. Furthermore, synthetic SMCs can reacquire a contractile phenotype, which is referred to as redifferentiation[6-8], indicating that phenotypic switching can occur in both directions.
Delineating these pathways is important for understanding the functional differences in healthy or diseased/aged blood vessels. Contractile SMCs, as the name suggests, contract and relax in response to biological cues to maintain vascular tone. Synthetic SMCs proliferate and migrate into the intima, which contributes to neointimal hyperplasia, progression of atherosclerosis, coronary microvascular dysfunction and many other pathologies. Therefore, identifying defective signaling pathways in SMCs that could be targeted by new or re-purposed therapies will have a major effect on global health, and societal and financial costs.
RhoA
RhoA is a member of the Rho subfamily of GTPases and has diverse roles within the cell, such as the regulation of morphology, cytoskeletal arrangement and migration. Recently recognized roles of RhoA are transcriptional control, reactive oxygen species production and the DNA damage response pathway in a cell-dependent context[9-11]. RhoA is post-translationally modified by the addition of geranylgeranyl pyrophosphate at the carboxyl terminus. The attachment of this moiety renders the protein lipophilic, and it is transported to cellular membranes to carry out its role[12].
Regulation of RhoA
Once in the membrane, the activity of RhoA is tightly controlled by a number of activatory and inhibitory mechanisms. Therefore, RhoA acts as a molecular switch cycling between an inactive guanosine diphosphate (GDP)-bound and an active guanosine triphosphate (GTP)-bound conformation, allowing interactions with downstream targets to trigger a cascade of cellular responses[13]. This tight regulation is important because over-activation of Rho proteins results in the pathogenesis of several cardiovascular disorders[14]. A combination of regulatory proteins is responsible for mediating RhoA activity, such as Rho guanine exchange factors (GEFs), GTPase-activating proteins (GAPs) and GDP dissociation inhibitors (GDIs).
GEFs
RhoGEFs promote GDP/GTP exchange to enable the formation of active GTP-bound RhoA[15]. A number of RhoGEFs have been identified as susceptibility genes for cardiovascular disorders. The role of RhoGEFs, specifically leukemia-associated Rho GEF, PDZ domain-containing RhoGEF and p115 RhoGEF, in activating Rho proteins allows for the modulation of vascular tone, particularly in hypertension[16]. GEF-H1, which is a RhoA-specific GEF associated with cytoskeletal structure, microtubules and actin cytoskeletal regulation, induces the activation of RhoA. In SMCs, p115 RhoGEF and GEF-H1 promote SMC proliferation[17]. The dual nature of RhoA activation, where it can promote both differentiation and dedifferentiation, is discussed in the “RhoA and SMC phenotype” section below.
GAPs
RhoGAPs are negative regulators of RhoA[18] and are responsible for increasing or stimulating the hydrolysis of RhoGTPases. RhoGAPs trigger the intrinsic GTPase activity that RhoA possesses to hydrolyze the bound GTP back into GDP, switching off the signaling mechanism[15]. Even though RhoGAPs are widely expressed, each of them plays a specialized role, and they regulate RhoGTPase signals spatially and temporally by detecting their expression patterns, domain structures and potential protein interactions[19]. RhoA is targeted specifically by p122RhoGAP and RARhoGAP[20]. Additionally, in SMCs, RhoA can trigger RhoA/Rho kinase (ROCK)-dependent inhibition of myosin phosphatase and subsequent cellular migration[21-24].
GDIs
RhoGDIs sequester RhoA in the cytoplasm. RhoGDIs prevent the correct localization of RhoA to cellular membranes, and also prevent the dissociation of GDP from RhoA, ensuring that GTP cannot bind and trigger the signaling cascade. RhoGDIs act to couple the nucleotide cycle of the Rho family GTPases to a membrane cycle with localized G protein for signaling[25]. There are three isoforms for RhoGDIs, namely RhoGDI1, RhoGDI2 and RhoGDI3, and the former two are cytosolic and the latter is non-cytosolic[26]. RhoGDIs appear to lack specific sequences that confer direct membrane association[27]. However, they are still considered an important target for druggable therapeutics within signaling mechanisms controlled by G proteins, and inhibiting RhoGDIs could have profound effects on cellular activity[28].
MicroRNAs
While RhoGEFs, GAPs and GDIs act at the post-translational level, RhoA can also be regulated at the post-transcriptional level by microRNAs (miRNAs). These short, non-coding RNAs are associated with cardiovascular diseases and SMC phenotypic switching[29]. They negatively regulate target protein translation by binding to mRNA and targeting it for degradation. A number of miRNAs are known to target RhoA mRNA, such as miR-31, miR-200b and miR-340[30-33]. Therefore, these miRNAs can inhibit the RhoA signaling pathway by reducing the absolute amount of RhoA present within a cell instead of regulating its activity level. A comprehensive understanding of RhoA-targeting miRs specifically in vascular SMCs has yet to be achieved. However, miR-133a and miR-141[34,35] have been validated in a number of vascular SMC types, and most recently, miR-145 has been suggested to regulate RhoA[36]. Whether this is a direct or indirect targeting remains to be determined, but because of the importance of miR-145 in regulating the SMC phenotype and function[29], this is worthy of further investigation.
A summary of the various RhoA regulatory mechanisms is shown in Figure 1.
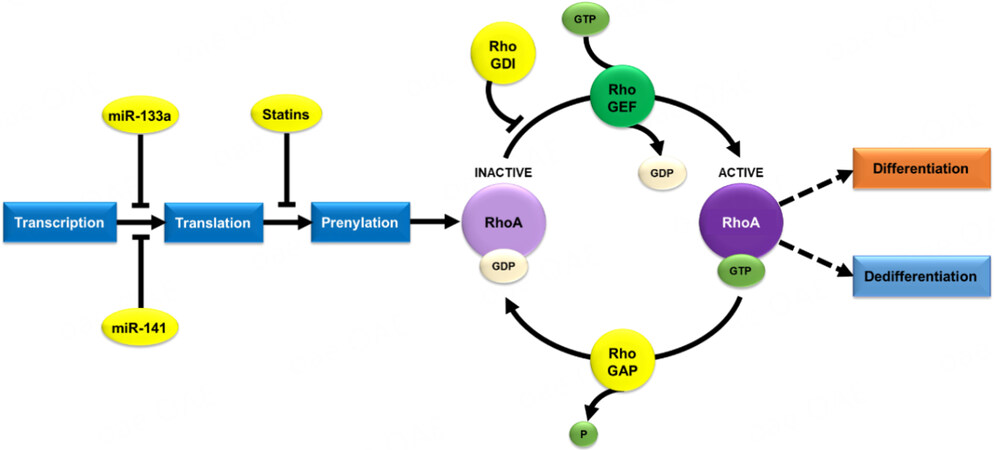
Figure 1. Post-transcriptional regulation of RhoA in smooth muscle cells. RhoA activity is dependent on GTP and is inactive when bound to GDP. A number of protein families regulate this activation cycle, such as RhoGEFs, RhoGAPs and RhoGDIs. RhoA can also be post-transcriptionally regulated by the microRNAs miR-133a and miR-141, and post-translationally by statins. GTP: Guanosine triphosphate; GDP: guanosine diphosphate; GEF: guanine exchange factor; GAP: GTPase-activating protein; GDI: guanine dissociation inhibitor;
RhoA AND SMC PHENOTYPE
Because of the critical role that RhoA plays in regulating morphology, migration and the cytoskeleton, alterations in RhoA activity will inevitably have an effect on SMC biology. However, the manner in which RhoA has an effect - through contractility or migration - remains controversial and is dependent upon a stimulus. The principal effector proteins of the RhoA signaling pathway are the ROCKs.
The ROCKs are serine/threonine kinases and consist of two isoforms, namely ROCK1 (also known as ROCK-beta or p160 ROCK) and ROCK2 (also known as ROCK-alpha or p150 ROCK)[37-39]. ROCK1 and ROCK2 share a similar structure with 92% homology in their kinase domains. They also share pleckstrin-homology domains, which enable protein interactions, and carboxy-terminal domains, which act as auto-inhibitors to regulate their kinase activity[21]. Active GTP-bound RhoA binds to the Rho-binding domain in ROCKs to induce a conformational change in the protein, which allows it to phosphorylate downstream effectors[40].
Both ROCK isoforms are expressed ubiquitously in invertebrates and vertebrates. However, within the vasculature, ROCK2 expression is proportionally higher in vascular endothelial cells and SMCs, and ROCK1 is the dominant isoform in circulatory inflammatory cells[41,42]. Nonetheless, many studies have focused on the ROCK1 isoform and its critical role in stress fiber and focal adhesion formation, as well as SMC contraction[43].
Promotion of the contractile (differentiated) SMC phenotype
RhoA/ROCK promotes the contractile SMC phenotype through the stabilization of actin stress fibers. These fibers are composed of actin filaments held together by the actin crosslinking protein α-actinin and are responsible for maintaining cell shape and adhesion. Actin stress fibers are essential in mediating cell migration and interactions with the environment[44]. RhoA can be activated by transforming growth factor beta (TGFβ; a well-recognized differentiation stimulus) or G protein-coupled receptors and signals through the ROCK and mammalian diaphanous-related formin pathways to promote stress fiber formation. ROCKs can directly activate myosin light chain kinase to stabilize stress fibers. ROCKs also stimulate LIM kinase to phosphorylate cofilin. Cofilin promotes destabilization of stress fibers and its phosphorylation by LIM kinase removes this function[45,46]. In contrast, mammalian diaphanous-related formin activates profilin, which has a counter role to cofilin[47]. In rat podocyte C7 cells, afadin is required for RhoA/ROCK-dependent stress fiber formation, and its depletion leads to downregulation of RhoA/ROCK activity and, consequently, loss of actin stress fibers[48].
In addition to the stabilization of stress fibers, RhoA mediates SMC differentiation by regulating SRF-dependent transcription, which is responsible for the coordinated expression of several smooth muscle-specific contractile and cytoskeletal genes[4]. The stabilized stress fibers promote the transfer of MRTF-A into the nucleus where it can then associate with SRF to upregulate classical differentiated SMC markers[49,50]. Indeed, the inhibition of either RhoA or ROCK impairs the expression of α-SMA and smooth muscle 22 alpha[51].
Promotion of the synthetic (dedifferentiated) SMC phenotype
The RhoA/ROCK signaling pathway also promotes dedifferentiation of SMCs through mediating migratory responses to a host of pro-proliferative and pro-migratory stimuli. One of the most well-recognized dedifferentiation stimuli, PDGF-BB, acts in part by activating RhoA. The RhoA/ROCK axis can also be upregulated by pro-synthetic stimuli, such as lysophosphatidic acid[52] and angiotensin II[53].
PDGF-BB upregulates the activation of RhoA, ROCK1 and ROCK2 in rabbit and human aortic vascular SMCs[54,55]. The activation of ROCK1 and ROCK2 is responsible for promoting cell cycle progression via transcriptional regulation of cyclins, whereas ROCK1 alone is responsible for the pro-migratory effect of PDGF-BB. Interestingly, the RhoA pathway also upregulates the expression of PDGF receptor beta to promote persistent dedifferentiation through positive feedback of the PDGF signal[55].
Integrins are transmembrane receptors, which are responsible for linking the cell cytoskeleton to the extracellular matrix, and this accounts for SMC phenotypic changes[56]. Integrin αVβ3 activates RhoA through the tyrosine kinase pathway to mediate directional migration[57]. This integrin is weakly expressed in contractile SMCs, but is activated in response to vitronectin, osteopontin and fibronectin[58]. Because these extracellular matrix proteins can be expressed by synthetic SMCs, this may be another mechanism (in addition to PDGF-BB) that prolongs the dedifferentiated phenotype.
This dual role of RhoA, where it promotes the contractile and synthetic phenotypes, supports the hypothesis that RhoA is a critical regulator of the SMC phenotypic fate, which can be protective against or causative of vascular disease depending upon its context [Figure 2]. The mechanisms controlling this dedifferentiation and redifferentiation of SMCs are unclear, but several molecular pathways that control SMC modulation are likely to be involved. The involvement of RhoA/ROCK in phenotypic switching could, at least in part, account for redifferentiation and possibly involve a complex interaction between several biomarkers. However, the critical role of RhoA/ROCK in SMC redifferentiation is yet to be fully understood.

Figure 2. Regulation of smooth muscle cell phenotypes. Smooth muscle cells usually exist in a contractile differentiated state characterized by expression of contractile proteins, such as α-SMA, SM22-α, calponin and smoothelin. This is regulated by the SRF-myocardin transcription complex in response to extracellular and intracellular cues. Dedifferenitation into a synthetic phenotype is driven by the inhibition of the SRF-myocardin system via KLF4. RhoA and ROCKs play a role in both of these pathways. α-SMA: Alpha smooth muscle actin; ECM: extracellular matrix; GPCR: G protein-coupled receptor; KLF4: Kruppel-like factor 4; LIMK: LIM domain kinase; mDia: mammalian diaphanous-related formin; MLC: myosin light chain; MRTF: myocardin-related transcription factor; NFκB: nuclear factor kappa B; PDGF-BB: platelet-derived growth factor-BB; PDGF-Rβ: platelet-derived growth factor-BB receptor beta; RGS: regulator of G protein signaling; ROCK: Rho kinase; SM22-α: smooth muscle 22 alpha; SRF: serum-response factor; TGFβ: transforming growth factor beta; TGFBRII: transforming growth factor beta receptor two.
RhoA AND POST-REVASCULARIZATION COMPLICATIONS IN DIABETES
Patients with T2DM present with microvascular and macrovascular complications[59]. Both of these complications have similar etiological characteristics, and chronic hyperglycemia is an important factor for their initiation. Microvascular complications include nephropathy, neuropathy and retinopathy[60]. The macrovascular complications of T2DM are underpinned by widespread atherosclerotic plaque formation in coronary, carotid, renal, and other large and medium-sized arteries[61]. Diabetes is an independent risk factor for cardiovascular disease. The prevalence of cardiovascular disease in patients with T2DM is 2-4 times higher than that in non-diabetic patients[62]. While intensive glycemic control can reverse microvascular complications fully, this does not occur for macrovascular complications, at least in the medium term[63]. Consequently, many patients with T2DM require surgical intervention to restore adequate blood flow to the heart.
Coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) are used to revascularize the heart. Although PCI is more common, approximately 15,000 CABG surgeries are performed annually in the UK[64]. CABG has lower associated mortality and morbidity risks than PCI[65], and is more beneficial for patients with T2DM and complex vessel disease[66,67]. While only approximately 10% of people have diabetes[68], more than 40% of patients undergoing CABG have T2DM[69]. Therefore, CABG will continue to be a necessity over the coming years. Saphenous vein (SV) grafts have much poorer patency than arterial grafts[70]. However, because of the extensive nature of coronary disease in patients with T2DM, SV grafts are commonly the conduit of choice[71]. Unfortunately, the failure rate of these grafts remains high, and maladaptive histological changes indicate that only 40%-50% of grafts remain patent after 10 years[72,73]. Additionally, diabetes is an independent risk factor for higher mortality of repeat revascularization[74].
Adaptation and arterialization of vascular grafts
Following the implantation of SV grafts into the coronary circulation, these grafts must undergo a process of arterialization to withstand the greater mechanical forces and pressure of the myocardium, as opposed to their normal position in the leg. During the first few days post-CABG, dedifferentiation of medial SMCs at the site of anastomoses and intimal injury occurs with an associated increase in proliferative activity[75,76]. Intimal hyperplasia resulting from enhanced proliferative and migratory activity appears to be an initial, adaptive response of a SV graft into the arterial circulation and is positive for graft integration[77,78].
This switch to the synthetic phenotype is also transient, and dedifferentiated SMCs must redifferentiate into the contractile phenotype in a timely manner to form a fully functioning conduit without progressing into maladaptive neointimal hyperplasia[6,76]. Elevated glucose concentrations can induce prenylation and RhoA activity in rodents. However, the implications of this finding for post-bypass adaptation are yet to be studied[79,80].
SMCs from the SV of patients with T2DM show a mixed phenotype that has features of contractile and synthetic cells. SMCs in T2DM tend to have increased levels of α-SMA and miR-145 and a reduced proliferative capacity indicative of contractile SMCs. SMCs in T2DM also have an enlarged rhomboid shape, defective F-actin cytoskeleton and secretory profile, which is suggestive of the synthetic phenotype[81-84]. Importantly, primary human SV SMCs from patients with T2DM consistently show downregulated RhoA protein and activity levels, which are post-transcriptionally controlled. This finding is specific to the SV because SMCs from arterial conduits (internal mammary artery) have no such impairment[84]. Internal mammary artery arterial grafts are not prone to the same failure rate as that in the SV. Therefore, the basally-reduced level of RhoA activity in these cells may prevent them from being able to adapt and dynamically switch their phenotype once implanted into coronary vessels.
Atherogenesis and intimal hyperplasia
In the process of atherogenesis, RhoA plays a major role in the modification of SMCs from a contractile to synthetic phenotype, leading to intimal thickening within the walls of the vessel. Studies on the effects of RhoA on macrophage behavior indicated that an increase in plasma cholesterol concentrations interfered with RhoA activation and inhibited macrophage migration, which was related to reduced generation of contractile force in the cells[85]. This finding provides a possible explanation for lipid-laden cell retention in most atherosclerotic lesions and the likely involvement of RhoA in cellular apoptosis. An elegant murine study examined the contribution of venous and arterial cells to intimal lesions 42 days post-bypass[86]. This study showed that both SMC sources contributed to intimal formation at the anastomoses, but intimal formation within the middle of the grafts was exclusively derived from the implanted vein. These findings highlight the critical importance of timely redifferentiation within the vein to form an optimally-functioning conduit. RhoA expression and regulation differ in T2DM according to a venous or arterial source[84], and understanding the activity of RhoA in these scenarios would be beneficial.
Within SV SMCs, the activation of RhoA and ROCKs promote the synthetic phenotype via the orphan G-protein coupled receptor GPR35, which causes an increase in stress fibers and cell length. This situation leads to a subsequent increase in synthetic SMC migratory capacity[87] and contributes to intimal thickening. Interestingly, GPR35 is reportedly anti-inflammatory in the majority of cell types tested[88], although notably, SMCs have not yet been examined in this regard. The upregulation of RhoA is also essential for the synthesis of RGS5, which is required to promote the synthetic SMC phenotype, and this allows for the structural renovation of the arterial wall[89].
During atherogenesis, there is an accumulation of various cell types within the vessel wall, which include pericyte-like stellate cells. These cells are found immediately below the endothelial lining[90,91]. Pericytes are structurally similar to SMCs in that they are composed of contractile filaments such as α-SMA. Indeed, the shared characteristics between SMCs and pericytes could make the latter susceptible to the interference of RhoA, specifically the GEF1 activator, which is responsible for mediating α-SMA[92]. Pericyte-like cells are highly variable and show a flexible phenotype. Therefore, pericyte-like cells are yet to be properly classified, with some studies suggesting that they are an adaptive group of cells, and express markers variably depending on their environment[90]. This attribute causes difficulty in predicting a likely effect of RhoA (de)regulation on these cells and determining how it may compare with classical SMC regulation.
In addition to reduced baseline RhoA activity, SV SMCs in T2DM are exposed to a number of circulating and surrounding factors that provide competing phenotypic cues. Pro-contractile stimuli, such as TGFβ, are enhanced in T2DM[93]. However, in contrast, pro-synthetic extracellular matrix proteins, such as fibronectin and osteopontin, are increased in response to increased advanced glycation end-products and deregulated calcium signaling in T2DM[94,95].
RhoA AND STATINS
Statins are 3-hydroxy-3-methylglutaryl-Coenzyme A reductase inhibitors. They are principally prescribed owing to their cholesterol-lowering ability, but also exhibit beneficial pleiotropic effects, such as improvement of endothelium-dependent vessel relaxation, attenuated atherosclerotic progression and a reduced incidence of heart failure[96]. The mechanisms underpinning these pleiotropic effects are incompletely understood, although they likely involve, at least in part, alteration of RhoA signaling in vascular cells[97].
The inhibition of the mevalonate pathway (responsible for cholesterol biosynthesis) also inhibits geranylgeranylation and farnesylation, and consequently reduces prenylation of proteins such as RhoA, inhibiting their activity[98]. Fluvastatin blocks lipoprotein(a)-induced RhoA activity in human SMCs, negating the detrimental effects of lipoprotein(a) on vascular remodeling[57]. Similarly, fluvastatin inhibits PDGF-induced proliferation in rodent SMCs via the inhibition of RhoA, preventing transition to a synthetic phenotype and aberrant vascular remodeling[99]. Simvastatin treatment permanently impairs adrenergic α-agonist-induced contractility through the blockade of voltage-operated calcium channels and the inhibition of RhoA-induced myosin light chain phosphorylation[100]. While these signalling events are all conceptually beneficial for vessel function by promoting vasodilation and reducing remodeling, they also possess undesirable effects. Simvastatin promotes SMC apoptosis and reduces the lumen area[100], which is associated with cytoskeletal integrity. The pro-apoptotic factor Bmf is usually sequestered on stable actin fibers. When statin use impairs RhoA, this reduces the stability of actin fibers, and Bmf is released and translocated to the mitochondria and then induces an apoptotic cascade[101].
Implications for statin use in patients with T2DM
The importance of statins is intimately associated with the vascular complications of T2DM. As discussed above, animal studies have shown that hyperglycemia increases RhoA activity and upregulates SMC proliferation, and this is abrogated by pitavastatin treatment[79]. This finding suggests a positive role for statins in SMC hyperproliferative disorders caused by T2DM (e.g., neointimal hyperplasia and atherosclerosis). However, in human SV SMCs, there is an inherent inhibition of RhoA activity in unstimulated T2DM cells[84]. This would conceivably be reduced even further if these patients were treated with statins. The cumulative inhibition of RhoA through combining T2DM with statin use may explain why SV grafts in patients with T2DM still have such a poor patency rate, and is worthy of further investigation.
One controversial consequence of prolonged statin use is an increased risk of developing new-onset T2DM by 10%-45%[102]. This occurs via a two-pronged attack whereby certain statins cause pancreatic β-cell dysfunction through the inhibition of L-type calcium channels and glucose transporter 2 translocation, thus impairing insulin release. In parallel, statins increase insulin resistance through inhibiting insulin receptor substrate-1 and glucose transporter 4 translocation in peripheral tissues[97]. Notably, the relative cardiovascular benefit of statins outweighs the risk of new-onset diabetes[103]. However, the prescription of statins for secondary preventative care in patients who are already at a high risk of developing T2DM may facilitate its development, and the consequent cardiovascular-associated T2DM morbidity and mortality.
CONCLUSIONS
The healthcare and socioeconomic costs of escalating T2DM cannot be underestimated. While there have been major breakthroughs in restoring glycemic control and managing T2DM over the last few decades, macrovascular complications persist. Therefore, understanding the molecular pathways that affect the blood vessels of these patients is of utmost importance. The benefits of statins for cardiovascular patients are well recognized, but controversy still surrounds their widespread use. Because of the critical role that RhoA plays in SMC phenotypic switching, surprisingly, there have been no clinical studies regarding its potential as a therapeutic target. Therefore, these studies need to be performed to progress the field. The evidence discussed in this review highlights the important role of RhoA in maintaining the sensitivity of SMCs to respond to de/differentiation cues, and the downstream effects that this has on SMC function, and thus vascular health. We suggest that further research examining this role will link molecular, cellular and vascular changes and identify areas for intervention. Further research on the pleiotropic inhibition of RhoA activity by statins in patient groups where RhoA is already impaired is required. These studies are important to establish if additional therapies restoring RhoA in SMCs, especially in implanted coronary conduits, could improve revascularization outcomes.
DECLARATIONS
Authors’ contributionsConceptualized the article: Riches-Suman K
Both authors contributed equally to the content of the article.
Availability of data and materialsNot applicable.
Financial support and sponsorshipAsare-Amankwah Y is supported by the Ghana Scholarships Secretariat.
Conflicts of interestBoth authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health 2020;10:107-11.
2. Dal Canto E, Ceriello A, Rydén L, et al. Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol 2019;26:25-32.
3. Riches-Suman K, Hussain A. Identifying and targeting the molecular signature of smooth muscle cells undergoing early vascular ageing. Biochim Biophys Acta Mol Basis Dis 2022;1868:166403.
4. Mack CP. Signaling mechanisms that regulate smooth muscle cell differentiation. Arterioscler Thromb Vasc Biol 2011;31:1495-505.
6. Beamish JA, He P, Kottke-Marchant K, Marchant RE. Molecular regulation of contractile smooth muscle cell phenotype: implications for vascular tissue engineering. Tissue Eng Part B Rev 2010;16:467-91.
7. Christen T, Verin V, Bochaton-piallat M, et al. Mechanisms of neointima formation and remodeling in the porcine coronary artery. Circulation 2001;103:882-8.
8. Kocher O, Gabbiani F, Gabbiani G, et al. Phenotypic features of smooth muscle cells during the evolution of experimental carotid artery intimal thickening. Biochemical and morphologic studies. Lab Invest 1991;65:459-70.
9. Cheng C, Seen D, Zheng C, Zeng R, Li E. Role of small GTPase RhoA in DNA damage response. Biomolecules 2021;11:212.
10. Ngo ATP, Parra-Izquierdo I, Aslan JE, McCarty OJT. Rho GTPase regulation of reactive oxygen species generation and signalling in platelet function and disease. Small GTPases 2021;12:440-57.
11. Tkach V, Bock E, Berezin V. The role of RhoA in the regulation of cell morphology and motility. Cell Motil Cytoskeleton 2005;61:21-33.
12. Solski PA, Helms W, Keely PJ, Su L, Der CJ. RhoA biological activity is dependent on prenylation but independent of specific isoprenoid modification. Cell Growth Differ 2002;13:363-73.
13. Guan R, Xu X, Chen M, et al. Advances in the studies of roles of Rho/Rho-kinase in diseases and the development of its inhibitors. Eur J Med Chem 2013;70:613-22.
14. Loirand G, Scalbert E, Bril A, Pacaud P. Rho exchange factors in the cardiovascular system. Curr Opin Pharmacol 2008;8:174-80.
15. Loirand G, Rolli-Derkinderen M, Pacaud P. RhoA and resistance artery remodeling. Am J Physiol Heart Circ Physiol 2005;288:H1051-6.
16. Li M, Jiao Q, Xin W, et al. The emerging role of Rho guanine nucleotide exchange factors in cardiovascular disorders: insights into atherosclerosis: a mini review. Front Cardiovasc Med 2021;8:782098.
17. Yu L, Quinn DA, Garg HG, Hales CA. Heparin inhibits pulmonary artery smooth muscle cell proliferation through guanine nucleotide exchange factor-H1/RhoA/Rho kinase/p27. Am J Respir Cell Mol Biol 2011;44:524-30.
18. Moon S. Rho GTPase-activating proteins in cell regulation. Trends in Cell Biology 2003;13:13-22.
19. Huang GH, Sun ZL, Li HJ, Feng DF. Rho GTPase-activating proteins: regulators of Rho GTPase activity in neuronal development and CNS diseases. Mol Cell Neurosci 2017;80:18-31.
20. Tcherkezian J, Lamarche-Vane N. Current knowledge of the large RhoGAP family of proteins. Biol Cell 2007;99:67-86.
21. Amano M, Chihara K, Nakamura N, Kaneko T, Matsuura Y, Kaibuchi K. The COOH terminus of Rho-kinase negatively regulates rho-kinase activity. J Biol Chem 1999;274:32418-24.
22. Kimura K, Ito M, Amano M, et al. Regulation of myosin phosphatase by Rho and Rho-associated kinase (Rho-kinase). Science 1996;273:245-8.
23. Loirand G, Pacaud P. The role of Rho protein signaling in hypertension. Nat Rev Cardiol 2010;7:637-47.
24. Mueller BK, Mack H, Teusch N. Rho kinase, a promising drug target for neurological disorders. Nat Rev Drug Discov 2005;4:387-98.
25. Garcia-Mata R, Boulter E, Burridge K. The “invisible hand”: regulation of RHO GTPases by RHOGDIs. Nat Rev Mol Cell Biol 2011;12:493-504.
26. Nagar H, Kim S, Lee I, et al. CRIF1 deficiency suppresses endothelial cell migration via upregulation of RhoGDI2. PLoS One 2021;16:e0256646.
27. Dovas A, Couchman JR. RhoGDI: multiple functions in the regulation of Rho family GTPase activities. Biochem J 2005;390:1-9.
28. Ahmad Mokhtar AMB, Ahmed SBM, Darling NJ, Harris M, Mott HR, Owen D. A complete survey of RhoGDI targets reveals novel interactions with atypical small GTPases. Biochemistry 2021;60:1533-51.
29. Riches-Suman K. Diverse roles of microRNA-145 in regulating smooth muscle (dys)function in health and disease. Biochem Soc Trans 2021;49:353-63.
30. Feng MB, Li GH, Dou FF. Long-chain non-coding RNA LOC554202 promotes proliferation, migration, and invasion of nasopharyngeal carcinoma cells by binding to microRNA-31 expression and regulating RhoA expression. Eur Rev Med Pharmacol Sci 2020;24:10550-6.
31. Korourian A, Roudi R, Shariftabrizi A, Madjd Z. MicroRNA-31 inhibits RhoA-mediated tumor invasion and chemotherapy resistance in MKN-45 gastric adenocarcinoma cells. Exp Biol Med 2017;242:1842-7.
32. Wang BG, Li JS, Liu YF, Xu Q. MicroRNA-200b suppresses the invasion and migration of hepatocellular carcinoma by downregulating RhoA and circRNA_000839. Tumour Biol 2017;39:1010428317719577.
33. Wang H, Guo W, Jian Q, et al. MicroRNA-340 inhibits squamous cell carcinoma cell proliferation, migration and invasion by downregulating RhoA. J Dermatol Sci 2018;92:197-206.
34. Li Y, Ouyang M, Shan Z, et al. Involvement of microRNA-133a in the development of arteriosclerosis obliterans of the lower extremities via RhoA targeting. J Atheroscler Thromb 2015;22:424-32.
35. Liu L, Zang J, Chen X, et al. Role of miR-124 and miR-141 in the regulation of vascular reactivity and the relationship to RhoA and Rac1 after hemorrhage and hypoxia. Am J Physiol Heart Circ Physiol 2016;310:H206-16.
36. Chung DJ, Wu YL, Yang MY, Chan KC, Lee HJ, Wang CJ. Nelumbo nucifera leaf polyphenol extract and gallic acid inhibit TNF-α-induced vascular smooth muscle cell proliferation and migration involving the regulation of miR-21, miR-143 and miR-145. Food Funct 2020;11:8602-11.
37. Fujisawa K, Fujita A, Ishizaki T, Saito Y, Narumiya S. Identification of the Rho-binding domain of p160ROCK, a Rho-associated coiled-coil containing protein kinase. J Biol Chem 1996;271:23022-8.
38. Loirand G, Guérin P, Pacaud P. Rho kinases in cardiovascular physiology and pathophysiology. Circ Res 2006;98:322-34.
39. Nakagawa O, Fujisawa K, Ishizaki T, Saito Y, Nakao K, Narumiya S. ROCK-I and ROCK-II, two isoforms of Rho-associated coiled-coil forming protein serine/threonine kinase in mice. FEBS Lett 1996;392:189-93.
40. Mong PY, Wang Q. Activation of Rho kinase isoforms in lung endothelial cells during inflammation. J Immunol 2009;182:2385-94.
41. Cheng C, Liu XB, Xu DL, Zhang J. Increased ROCK1 not ROCK2 in circulating leukocytes in rats with myocardial ischemia/reperfusion. Perfusion 2020;35:819-25.
42. Chevrier V, Piel M, Collomb N, et al. The Rho-associated protein kinase p160ROCK is required for centrosome positioning. J Cell Biol 2002;157:807-17.
43. van Nieuw Amerongen GP, van Hinsbergh VW. Cytoskeletal effects of Rho-like small guanine nucleotide-binding proteins in the vascular system. ATVB 2001;21:300-11.
44. Tojkander S, Gateva G, Lappalainen P. Actin stress fibers - assembly, dynamics and biological roles. J Cell Sci 2012;125:1855-64.
45. Maekawa M, Ishizaki T, Boku S, et al. Signaling from Rho to the actin cytoskeleton through protein kinases ROCK and LIM-kinase. Science 1999;285:895-8.
46. Leung T, Chen XQ, Manser E, Lim L. The p160 RhoA-binding kinase ROK alpha is a member of a kinase family and is involved in the reorganization of the cytoskeleton. Mol Cell Biol 1996;16:5313-27.
47. Watanabe N, Madaule P, Reid T, et al. p140mDia, a mammalian homolog of Drosophila diaphanous, is a target protein for Rho small GTPase and is a ligand for profilin. EMBO J 1997;16:3044-56.
48. Saito K, Shiino T, Kurihara H, Harita Y, Hattori S, Ohta Y. Afadin regulates RhoA/Rho-associated protein kinase signaling to control formation of actin stress fibers in kidney podocytes. Cytoskeleton 2015;72:146-56.
49. Miralles F, Posern G, Zaromytidou A, Treisman R. Actin dynamics control SRF activity by regulation of its coactivator MAL. Cell 2003;113:329-42.
50. Hill CS, Wynne J, Treisman R. The Rho family GTPases RhoA, Racl, and CDC42Hsregulate transcriptional activation by SRF. Cell 1995;81:1159-70.
51. Mack CP, Somlyo AV, Hautmann M, Somlyo AP, Owens GK. Smooth muscle differentiation marker gene expression is regulated by RhoA-mediated actin polymerization. J Biol Chem 2001;276:341-7.
52. Ai S, Kuzuya M, Koike T, et al. Rho-Rho kinase is involved in smooth muscle cell migration through myosin light chain phosphorylation-dependent and independent pathways. Atherosclerosis 2001;155:321-7.
53. Qi Y, Liang X, Dai F, Guan H, Sun J, Yao W. RhoA/ROCK pathway activation is regulated by AT1 receptor and participates in smooth muscle migration and dedifferentiation via promoting actin cytoskeleton polymerization. Int J Mol Sci 2020;21:5398.
54. Pescatore LA, Bonatto D, Forti FL, Sadok A, Kovacic H, Laurindo FR. Protein disulfide isomerase is required for platelet-derived growth factor-induced vascular smooth muscle cell migration, Nox1 NADPH oxidase expression, and RhoGTPase activation. J Biol Chem 2012;287:29290-300.
55. Tang L, Dai F, Liu Y, et al. RhoA/ROCK signaling regulates smooth muscle phenotypic modulation and vascular remodeling via the JNK pathway and vimentin cytoskeleton. Pharmacol Res 2018;133:201-12.
56. Zhuge Y, Zhang J, Qian F, et al. Role of smooth muscle cells in cardiovascular disease. Int J Biol Sci 2020;16:2741-51.
57. Riches K, Franklin L, Maqbool A, et al. Apolipoprotein(a) acts as a chemorepellent to human vascular smooth muscle cells via integrin αVβ3 and RhoA/ROCK-mediated mechanisms. Int J Biochem Cell Biol 2013;45:1776-83.
58. Jain M, Chauhan AK. Role of integrins in modulating smooth muscle cell plasticity and vascular remodeling: from expression to therapeutic implications. Cells 2022;11:646.
59. Hayfron-Benjamin C, van den Born BJ, Maitland-van der Zee AH, et al. Microvascular and macrovascular complications in type 2 diabetes Ghanaian residents in Ghana and Europe: the RODAM study. J Diabetes Complications 2019;33:572-8.
60. Khanam PA, Hoque S, Begum T, Habib SH, Latif ZA. Microvascular complications and their associated risk factors in type 2 diabetes mellitus. Diabetes Metab Syndr 2017;11 Suppl 2:S577-81.
61. Jin J, Wang X, Zhi X, Meng D. Epigenetic regulation in diabetic vascular complications. J Mol Endocrinol 2019;63:R103-15.
62. Contreras F, Rivera M, Vasquez J, De la Parte MA, Velasco M. Diabetes and hypertension physiopathology and therapeutics. J Hum Hypertens 2000;14 Suppl 1:S26-31.
63. DM; DCCT/EDIC Research Group. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care 2014;37:9-16.
64. Ohri SK, Benedetto U, Luthra S, et al. Coronary artery bypass surgery in the UK, trends in activity and outcomes from a 15-year complete national series. Eur J Cardiothorac Surg 2022;61:449-56.
65. Spadaccio C, Benedetto U. Coronary artery bypass grafting (CABG) vs. percutaneous coronary intervention (PCI) in the treatment of multivessel coronary disease: quo vadis? Ann Cardiothorac Surg 2018;7:506-15.
66. d’Entremont MA, Yagi R, Salia SJS, et al. The effect of diabetes on surgical versus percutaneous left main revascularization outcomes: a systematic review and meta-analysis. J Cardiothorac Surg 2022;17:61.
67. Head SJ, Milojevic M, Daemen J, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. Lancet 2018;391:939-48.
69. Raza S, Sabik JF 3rd, Ainkaran P, Blackstone EH. Coronary artery bypass grafting in diabetics: a growing health care cost crisis. J Thorac Cardiovasc Surg 2015;150:304-2.e2.
70. Royse A, Pamment W, Pawanis Z, et al. Patency of conduits in patients who received internal mammary artery, radial artery and saphenous vein grafts. BMC Cardiovasc Disord 2020;20:148.
71. Ak E, Ak K, Midi A, et al. Histopathologic evaluation of saphenous vein grafts in patients with type II diabetes mellitus undergoing coronary artery bypass grafting. Cardiovasc Pathol 2021;52:107328.
72. Martínez-González B, Reyes-Hernández CG, Quiroga-Garza A, et al. Conduits used in coronary artery bypass grafting: a review of morphological studies. Ann Thorac Cardiovasc Surg 2017;23:55-65.
73. Raza S, Blackstone EH, Houghtaling PL, et al. Influence of diabetes on long-term coronary artery bypass graft patency. J Am Coll Cardiol 2017;70:515-24.
74. Maltais S, Widmer RJ, Bell MR, et al. Reoperation for coronary artery bypass grafting surgery: outcomes and considerations for expanding interventional procedures. Ann Thorac Surg 2017;103:1886-92.
75. Sasaki Y, Suehiro S, Becker AE, Kinoshita H, Ueda M. Role of endothelial cell denudation and smooth muscle cell dedifferentiation in neointimal formation of human vein grafts after coronary artery bypass grafting: therapeutic implications. Heart 2000;83:69-75.
76. Kockx MM, Cambier BA, Bortier HE, De Meyer GR, Van Cauwelaert PA. The modulation of smooth muscle cell phenotype is an early event in human aorto-coronary saphenous vein grafts. Virchows Arch A Pathol Anat Histopathol 1992;420:155-62.
77. Davies MG, Hagen PO. Structural and functional consequences of bypass grafting with autologous vein. Cryobiology 1994;31:63-70.
78. Muto A, Model L, Ziegler K, Eghbalieh SD, Dardik A. Mechanisms of vein graft adaptation to the arterial circulation: insights into the neointimal algorithm and management strategies. Circ J 2010;74:1501-12.
79. Ishiko K, Sakoda T, Akagami T, et al. Hyperglycemia induced cell growth and gene expression via the serum response element through RhoA and Rho-kinase in vascular smooth muscle cells. Prep Biochem Biotechnol 2010;40:139-51.
80. Chen GP, Zhang XQ, Wu T, Li L, Han J, Du CQ. Alteration of mevalonate pathway in proliferated vascular smooth muscle from diabetic mice: possible role in high-glucose-induced atherogenic process. J Diabetes Res 2015;2015:379287.
81. Hemmings KE, Riches-Suman K, Bailey MA, O’Regan DJ, Turner NA, Porter KE. Role of microRNA-145 in DNA damage signalling and senescence in vascular smooth muscle cells of type 2 diabetic patients. Cells 2021;10:919.
82. Madi HA, Riches K, Warburton P, O’Regan DJ, Turner NA, Porter KE. Inherent differences in morphology, proliferation, and migration in saphenous vein smooth muscle cells cultured from nondiabetic and Type 2 diabetic patients. Am J Physiol Cell Physiol 2009;297:C1307-17.
83. Riches K, Alshanwani AR, Warburton P, et al. Elevated expression levels of miR-143/5 in saphenous vein smooth muscle cells from patients with Type 2 diabetes drive persistent changes in phenotype and function. J Mol Cell Cardiol 2014;74:240-50.
84. Riches K, Warburton P, O'Regan DJ, Turner NA, Porter KE. Type 2 diabetes impairs venous, but not arterial smooth muscle cell function: possible role of differential RhoA activity. Cardiovasc Revasc Med 2014;15:141-8.
85. Nagao T, Qin C, Grosheva I, Maxfield FR, Pierini LM. Elevated cholesterol levels in the plasma membranes of macrophages inhibit migration by disrupting RhoA regulation. Arterioscler Thromb Vasc Biol 2007;27:1596-602.
86. Wu W, Wang C, Zang H, et al. Mature vascular smooth muscle cells, but not endothelial cells, serve as the major cellular source of intimal hyperplasia in vein grafts. Arterioscler Thromb Vasc Biol 2020;40:1870-90.
87. McCallum JE, Mackenzie AE, Divorty N, et al. G-protein-coupled receptor 35 mediates human saphenous vein vascular smooth muscle cell migration and endothelial cell proliferation. J Vasc Res 2015;52:383-95.
88. Oliveira de Souza C, Sun X, Oh D. Metabolic functions of G protein-coupled receptors and β-arrestin-mediated signaling pathways in the pathophysiology of type 2 diabetes and obesity. Front Endocrinol 2021;12:715877.
89. Arnold C, Demirel E, Feldner A, et al. Hypertension-evoked RhoA activity in vascular smooth muscle cells requires RGS5. FASEB J 2018;32:2021-35.
90. Ivanova EA, Bobryshev YV, Orekhov AN. Intimal pericytes as the second line of immune defence in atherosclerosis. World J Cardiol 2015;7:583-93.
91. Lechartier B, Berrebeh N, Huertas A, Humbert M, Guignabert C, Tu L. Phenotypic diversity of vascular smooth muscle cells in pulmonary arterial hypertension: implications for therapy. Chest 2022;161:219-31.
92. Tsapara A, Luthert P, Greenwood J, Hill CS, Matter K, Balda MS. The RhoA activator GEF-H1/Lfc is a transforming growth factor-beta target gene and effector that regulates alpha-smooth muscle actin expression and cell migration. Mol Biol Cell 2010;21:860-70.
93. Qiao YC, Chen YL, Pan YH, et al. Changes of transforming growth factor beta 1 in patients with type 2 diabetes and diabetic nephropathy: a PRISMA-compliant systematic review and meta-analysis. Medicine 2017;96:e6583.
94. Sakata N, Meng J, Takebayashi S. Effects of advanced glycation end products on the proliferation and fibronectin production of smooth muscle cells. J Atheroscler Thromb 2000;7:169-76.
95. Yang H, Chen XY, Kuang SJ, et al. Abnormal Ca2+ handling contributes to the impairment of aortic smooth muscle contractility in Zucker diabetic fatty rats. J Mol Cell Cardiol 2020;141:82-92.
97. Patel KK, Sehgal VS, Kashfi K. Molecular targets of statins and their potential side effects: Not all the glitter is gold. Eur J Pharmacol 2022;922:174906.
98. Bonetti P. Statin effects beyond lipid lowering - are they clinically relevant? Eur Heart J 2003;24:225-48.
99. Ouyang QF, Han Y, Lin ZH, Xie H, Xu CS, Xie LD. Fluvastatin upregulates the α 1C subunit of CaV1.2 channel expression in vascular smooth muscle cells via RhoA and ERK/p38 MAPK pathways. Dis Markers 2014;2014:237067.
100. Kang S, Woo HH, Kim K, et al. Dysfunction of vascular smooth muscle and vascular remodeling by simvastatin. Toxicol Sci 2014;138:446-556.
101. Kang S, Kim K, Noh JY, et al. Simvastatin induces the apoptosis of normal vascular smooth muscle through the disruption of actin integrity via the impairment of RhoA/Rac-1 activity. Thromb Haemost 2016;116:496-505.
102. Yandrapalli S, Malik A, Guber K, et al. Statins and the potential for higher diabetes mellitus risk. Expert Rev Clin Pharmacol 2019;12:825-30.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Asare-Amankwah Y, Riches-Suman K. The complex role of RhoA in regulating vascular smooth muscle cell phenotype in Type 2 diabetes. Vessel Plus 2022;6:64. http://dx.doi.org/10.20517/2574-1209.2022.26
AMA Style
Asare-Amankwah Y, Riches-Suman K. The complex role of RhoA in regulating vascular smooth muscle cell phenotype in Type 2 diabetes. Vessel Plus. 2022; 6: 64. http://dx.doi.org/10.20517/2574-1209.2022.26
Chicago/Turabian Style
Asare-Amankwah, Yaw, Kirsten Riches-Suman. 2022. "The complex role of RhoA in regulating vascular smooth muscle cell phenotype in Type 2 diabetes" Vessel Plus. 6: 64. http://dx.doi.org/10.20517/2574-1209.2022.26
ACS Style
Asare-Amankwah, Y.; Riches-Suman K. The complex role of RhoA in regulating vascular smooth muscle cell phenotype in Type 2 diabetes. Vessel Plus. 2022, 6, 64. http://dx.doi.org/10.20517/2574-1209.2022.26
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 8 clicks
Cite This Article 8 clicks

 Like This Article 37
likes
Like This Article 37
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.