
Improving future postoperative atrial fibrillation care: a 30,000-foot viewpoint
 0
0Abstract
Aim: In the United States (US), post-operative atrial fibrillation (POAF) is the most common complication following cardiac surgery. In order to understand the opportunities to improve POAF patients’ care, this “30,000 foot” review evaluated the professional society POAF database/registry definitions and guideline recommendations.
Methods: All US-based professional society organizations with an interventional cardiac database/registry and/or cardiac care guidelines were identified; from these, the POAF database definitions and guideline recommendations were evaluated using a content analysis approach.
Results: The Society of Thoracic Surgeons (STS) POAF definition was the most frequently referenced definition (21% of key references). Only 50% (n = 5/10) US cardiac surgery databases/registries included any POAF definition; compared to STS, the other five definitions required substantially more detailed documentation. Across eight guidelines, three different types of POAF recommendations were found: risk assessment (n = 3); prevention
Conclusion: Across ten professional societies, 50% had no POAF definition; of the remaining five, no POAF definitional consistency was found. Across the eight US-based professional society POAF-related guidelines, only anticoagulation was uniformly recommended. Given these “big picture” findings, professional societies are urged to work collaboratively to harmonize these divergent POAF definitions and consolidate their evidence-based guideline recommendations to improve future POAF patients’ quality of care.
Keywords
INTRODUCTION
Post-operative atrial fibrillation (POAF) occurs in 20%-50% of cardiac operations and 10%-30% of non-cardiac surgeries[1,2]. Despite this high POAF rate, there is an astonishing lack of consensus among professional societies on an official POAF definition and POAF patients’ management.
Over the last decade, POAF has garnered increased attention; POAF is associated with increased hospital length of stay and costs[3]. In spite of this POAF spotlight, persistent disparities exist as to how hospitals and clinicians identify, monitor, and manage patients with a POAF complication.
Brief history
In 1966, Dr. Avedis Donabedian published his landmark quality improvement framework, which is commonly used today to evaluate healthcare quality[4]. In 1992, the Department of Veterans Affairs (VA) health care system was the first health care organization to define and monitor surgical patients’ preoperative and postoperative atrial fibrillation[5]. Based on these historical VA endeavors, the STS in 2000 published their first POAF definition (i.e., adult cardiac surgery database, version 2.35), which has become the “gold standard” definition[4,6,7]. Since then, there have been many publications evaluating POAF’s impact on surgical patients’ clinical outcomes and resource utilization. Despite the initial VA and STS POAF definitional uniformity, there has been a growing divergence across the POAF definitions used by surgical society databases as well as the subsequent guidelines promulgated. Comparing the cardiothoracic versus non-cardiothoracic surgical society-based publications, this study documents the tremendous diversity of POAF definitions for the first time.
METHODS
For this qualitative content analysis, ten professional societies’ cardiac interventional database definitions and clinical guideline recommendations were analyzed. Societies were classified into procedural versus medical, based upon their specialization as listed below.
Cardiothoracic Interventional Societies (CT societies)
1. Society of Thoracic Surgeons (STS)[6]
2. American Association for Thoracic Surgery (AATS)[8]
3. Society for Cardiovascular Angiography and Interventions (SCAI)[9]
4. American College of Surgeons (ACS) NSQIP[10]
All other Interventions (non-CT)
5. American College of Cardiology (ACC)[11]
6. American Heart Association (AHA)[11]
7. Heart Rhythm Society (HRS)[11,12]
8. American College of Chest Physicians (ACCP)[2,13]
9. Heart Failure Society of America (HFSA)
10. European Society of Cardiology (ESC)[1]
Other than the ESC [which published this guideline in collaboration with several listed United States (US)-based societies], the focus was placed on US-based professional society guidelines and database definitions. The latest guidelines and database definitions were identified for each society as of July 2021. All Society-related manuscripts were found using a comprehensive literature search by analyzing all publications since the VA’s definition of POAF was first published in 1991. Additionally, a thorough Mesh search (completed as of May 28, 2021) included the following literature review search strategy:
(((“atrial fibrillation”[MeSH Terms]) OR (“atrial flutter”[MeSH Terms])) AND ((“cardiac surgical procedures”[MeSH Terms]) or (“cardiology”[MeSH Terms]) or (“cardiac catheterization”[MeSH Terms]))) and (“definition” or “defined”)
This search resulted in 340 articles which were thoroughly analyzed for inclusion of working and stated definition for POAF. [Figure 1] provides an overview of the process of inclusion, but only 21% (n = 71) of these articles contained any POAF definition.
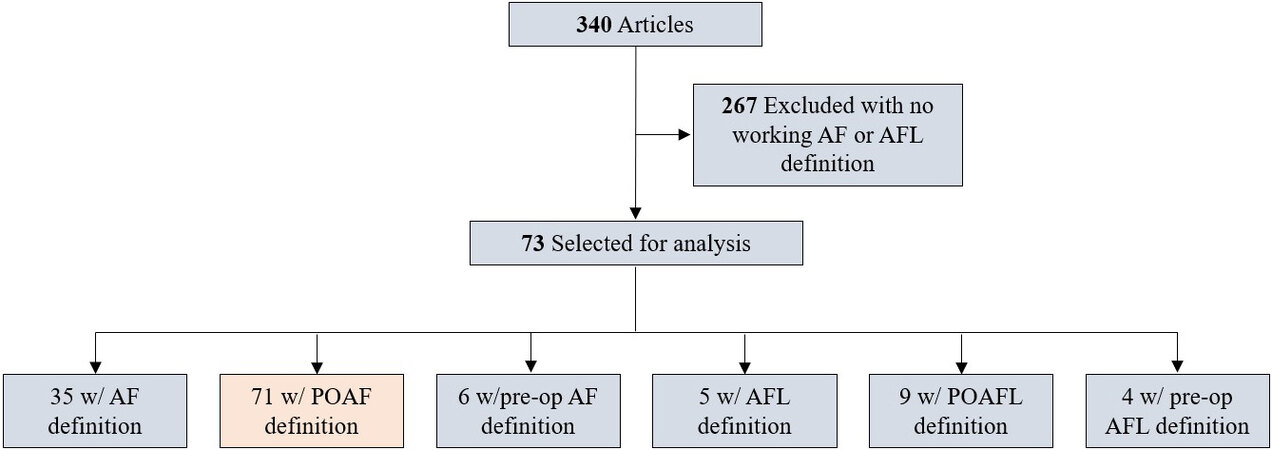
Figure 1. Hierarchal representation of our exclusion criteria for our article selection process. 71 w/ POAF definition in the highlighted box are the articles that were used in our analysis.
Qualitative content analysis was used to classify: (1) part I - all professional society-based POAF definitions; and (2) part II - all professional society-based POAF guideline recommendations; whenever possible, sub-component categories were developed to identify emerging themes.
For part I, the published POAF definitions from the 71 key reference manuscripts were compared to the professional society based POAF definitional components; these include the six characteristics associated with a POAF definition listed below (see Tables 1-3).
POAF characteristics
| Characteristics - subcomponents | STS | AATS | AHA ACC & HRS | ACS | SCAI | ACCP | HFSA | ESC | Count | |
| EKG finding | Absence of P waves | * | * | * | 3 | |||||
| Irregular RR intervals | * | * | * | 3 | ||||||
| Episode duration | < 30 s | * | 1 | |||||||
| > 30 s | * | 1 | ||||||||
| > 1 h | * | 1 | ||||||||
| First observation timing | New onset POAF: < 48 h | * | 1 | |||||||
| Persistent POAF: > 48 h | * | 1 | ||||||||
| Symptoms | Severe hypotension | * | * | 2 | ||||||
| Acute MI | * | 1 | ||||||||
| Ischemia | * | 1 | ||||||||
| Pulmonary edema/HF | * | * | 2 | |||||||
| Chest pain | * | 1 | ||||||||
| Syncope | * | 1 | ||||||||
| Asymptomatic | * | 1 | ||||||||
| General Def. | Clinically significant POAF: requires rhythm control, anti-coagulation, and/or extends hospitalization | * | 1 | |||||||
| New-onset POAF: working diagnosis in a patient w/o history of AF | * | 1 | ||||||||
| POAF definition: atrial fibrillation requiring treatment | * | 1 | ||||||||
| Inclusivity | Restrictive | * | * | * | 3 | |||||
| Inclusive | * | * | 2 | |||||||
| 3 | 11 | 0 | 8 | 0 | 2 | 0 | 2 |
Timing, nature, and treatment
| Criteria - subcomponents | Number of publications | |
| New-onset | Continuous AF at any time before discharge | 9 |
| Occurring during the procedure or within 30 days post-procedure | 6 | |
| Continuous AF at any time postoperatively | 4 | |
| Occurring during the procedure or within 30 days post-procedure, w/o history of previous AF | 2 | |
| Continuous AF of any duration at any time postoperatively | 2 | |
| Any documented AF in the first 7 days following surgery, w/o history of previous AF | 1 | |
| Any episodes that are brief, paroxysmal, and asymptomatic | 1 | |
| ICD-9 code discharge diagnosis code of AF, not present before admission | 1 | |
| Occurring during the procedure or within 3 days post-procedure | 1 | |
| Early onset | Occurring in the surgical department | 2 |
| Any AF episode diagnosed by a physician during the hospital stay | 1 | |
| ICD-9 code of 427.31 or ICD-10 code (I48.0, I48.1, I48.2, or I48.91) within admission or post-procedure | 1 | |
| Any documented AF in the first 6 days following surgery | 1 | |
| Any documented AF in the first 7 days following surgery | 1 | |
| Occurring during the procedure or within 14 days post-procedure | 1 | |
| Occurring during the procedure or within 9 days post-procedure | 1 | |
| Occurring during the procedure or within 10 days post-procedure | 1 | |
| Late-onset | Occurring 3 months after the procedure | 1 |
| Occurring during the rehabilitation period | 1 | |
| Occurring during rehabilitation period and within 20 ± 5 days | 1 | |
| (Transplant): occurring after discharge, minimum 14 days post-procedure, w/o history of previous AF | 1 | |
| (Transplant): occurring after discharge, minimum 9 days post-transplant, w/o history of previous AF | 1 | |
| Silent | Post-procedure, only detected by continuous ECG for pts w/o history of previous AF | 1 |
| Within 7 days post-procedure, only detected by Holter for pts w/o history of previous AF | 1 | |
| Recurrent | POAF recurrence: continuous AF at any time during or after the operation | 3 |
| Treatment | AF requiring treatment | 13 |
| Within 48 h post-procedure, confirmed by ECG, resulting in the need for intervention | 1 | |
| Any documented AF in the first 7 days following surgery and requiring treatment | 1 |
POAF imaging and duration
| Criteria - subcomponents | Number of publications | |
| EKG finding | Irregular RR intervals | 20 |
| Absence of P waves | 17 | |
| Fluctuating baseline | 4 | |
| No consistent P waves before QRS | 3 | |
| Episode duration | > 30 s | 22 |
| > 5 min | 14 | |
| > 10 min | 4 | |
| > 15 min | 3 | |
| > 30 min | 3 | |
| > 1 min | 2 | |
| > 60 min | 2 | |
| > 10 s | 1 | |
| > 2 min | 1 | |
| Several minutes | 1 | |
| < 5 min | 1 | |
| > 6 min | 1 | |
| > 10 min | 1 | |
| < 60 min | 1 | |
| > 12 h | 1 |
1. POAF electrocardiogram findings
2. POAF episode duration
3. Timing of the first POAF observation
4. POAF-related symptoms
5. General POAF definitions
(1) New-onset
(2) Early-onset
(3) Late-onset
(4) Silent
(5) Recurrent
(6) Treatment
6. Inclusivity
Evaluating these six POAF definitional characteristics, the ten professional societies’ POAF definitions were carefully analyzed (see Table 4).
Professional society POAF-related guidelines
| Criteria - subpopulation | STS | AATS | ACC AHA & ESC | ACS | SCAI | ACCP | HFSA | ESC | Count | |
| Have guidelines | * | * | * | * | * | * | 6 | |||
| Risks | Non-clinical risk factors* | * | * | * | 3 | |||||
| Clinical risk factors* | * | 1 | ||||||||
| Prevention | All patients* | * | * | * | * | 4 | ||||
| Higher risk patients* | * | * | * | 3 | ||||||
| Management | All patients* | * | * | * | 3 | |||||
| Anticoagulation* | * | * | * | * | * | * | 6 | |||
| Hemodynamically stable* | * | * | * | * | 4 | |||||
| Hemodynamically unstable* | * | * | * | * | 4 | |||||
| Rate control* | * | * | 2 | |||||||
| Rhythm control* | * | * | * | 3 | ||||||
| EF < 45% | * | 1 | ||||||||
| EF > 45% | * | 1 | ||||||||
| Medical | * | 1 | ||||||||
| EP catheterization | * | 1 | ||||||||
| Surgical treatment | * | 1 | ||||||||
| Non-pharmacologic | * | 1 | ||||||||
| Post discharge | * | 1 | ||||||||
| 7 | 15 | 9 | 6 | 0 | 3 | 0 | 5 |
For these same professional societies, their cardiac interventional guidelines were evaluated see [Table 4] according to the following three categories: POAF risk assessments, POAF prevention guidelines, and POAF management guidelines (see Tables 5-7).
POAF prevention guideline characteristics
| Subpopulation - subcomponents | STS | AATS | ACC AHA & ESC | ACS | SCAI | ACCP | HFSA | ESC | Count | ||
| All patients | Class I | Avoid B-blocker withdrawal | * | * | 2 | ||||||
| Treat pts undergoing cardiac surgery with prophylactic oral B-Blocker | * | * | 2 | ||||||||
| Class IIa | Diltiazem is reasonable in most patients undergoing major pulmonary resection who are not on B-blocker already | * | 1 | ||||||||
| Administer amiodarone prophylactically to cardiac surgery | * | * | * | 3 | |||||||
| Class IIb | Treat pts undergoing cardiac surgery with prophylactic oral B-Blocker | * | 1 | ||||||||
| Magnesium supplementation when Mg low or suspected body Mg low | * | * | 2 | ||||||||
| Class III | Digoxin is not recommended for prophylaxis | * | 1 | ||||||||
| Amiodarone is not recommended for patients undergoing pneumonectomy | * | 1 | |||||||||
| Flecainide is not recommended for prophylaxis | * | 1 | |||||||||
| Digitalis is not recommended for prophylaxis | * | 1 | |||||||||
| PVI is not recommended for the prevention of POAF if no previous AF history | * | 1 | |||||||||
| Higher risk | Class I | Chronic AF whom it is thought to continue post-operatively, anticoagulation is recommended | * | 1 | |||||||
| Class IIa | Administer amiodarone prophylactically to cardiac surgery | * | 1 | ||||||||
| Administer diltiazem prophylactically to POAF pts not taking B-Blocker | * | 1 | |||||||||
| Administer amiodarone prophylactically to pulmonary resection | * | 1 | |||||||||
| Class IIb | Administer sotalol prophylactically to cardiac surgery | * | 1 | ||||||||
| Administer IV Amiodarone prophylactically to esophagectomy | * | 1 | |||||||||
| Administration of colchicine may be considered postoperatively | * | 1 | |||||||||
| Administer Atorvastatin prophylactically in higher risk thoracic surgical procedures | * | 1 | |||||||||
| LAA excision during left lung surgery for pts w/ previous AF History | * | 1 | |||||||||
| 8 | 9 | 5 | 0 | 0 | 1 | 0 | 2 |
POAF patient risk characteristics
| Characteristics - subcomponents | STS | AATS | ACC AHA & ESC | ACS | SCAI | ACCP | HFSA | ESC | Count | ||
| Modifiable | HTN | * | * | 2 | |||||||
| Alcohol | * | 1 | |||||||||
| Smoking | * | 1 | |||||||||
| Obesity | * | 1 | |||||||||
| Exercise | * | 1 | |||||||||
| Non-modifiable | Cardiac | Preoperative atrial arrhythmias | * | * | * | * | 4 | ||||
| Valvular disease | * | * | * | 3 | |||||||
| Congestive HF | * | * | * | 2 | |||||||
| Pericarditis | * | * | 1 | ||||||||
| Ischemic heart disease | * | 1 | |||||||||
| MI | * | 1 | |||||||||
| Increased pulse pressure | * | 1 | |||||||||
| Peripheral arterial disease | * | 1 | |||||||||
| Left ventricular hypertrophy | * | 1 | |||||||||
| Left atrial enlargement | * | 1 | |||||||||
| Prior cardiac surgery | * | * | 1 | ||||||||
| Non-cardiac | Age | * | * | * | * | 4 | |||||
| Male gender | * | * | * | 3 | |||||||
| Chronic lung disease | * | * | 2 | ||||||||
| Elevated post op adrenergic tone | * | 1 | |||||||||
| Family history | * | 1 | |||||||||
| Genetic variants | * | 1 | |||||||||
| Discontinuation of beta blocker | * | 1 | |||||||||
| Digoxin | * | 1 | |||||||||
| Sepsis | * | 1 | |||||||||
| Shock | * | 1 | |||||||||
| Asthma | * | 1 | |||||||||
| Obstructive sleep apnea | * | 1 | |||||||||
| Pneumonia | * | 1 | |||||||||
| Pulmonary emboli | * | 1 | |||||||||
| Chronic renal failure | * | 1 | |||||||||
| Hyperthyroidism | * | * | 1 | ||||||||
| Procedures | Low risk (< 5% incidence) | Flexible bronchoscopy w/ or w/o biopsy | * | 1 | |||||||
| Photodynamic therapy | * | 1 | |||||||||
| Tracheal stenting | * | 1 | |||||||||
| Placement of thoracostomy tube | * | 1 | |||||||||
| Pleuroscopy, pleurodesis, decortication | * | 1 | |||||||||
| Tracheostomy | * | 1 | |||||||||
| Rigid bronchoscopy | * | 1 | |||||||||
| Mediastinoscopy | * | 1 | |||||||||
| Thoracoscopic lobectomy | * | 1 | |||||||||
| Thoracoscopic wedge resection | * | 1 | |||||||||
| Bronchoscopic laser surgery | * | 1 | |||||||||
| Esophagoscopy/PEG/esophageal dilation or stenting | * | 1 | |||||||||
| Intermediate risk (5%-15% incidence) | Thoracoscopic sympathectomy | * | 1 | ||||||||
| Segmentectomy | * | 1 | |||||||||
| Laparoscopic Nissen fundoplication/myotomy | * | 1 | |||||||||
| Zenker diverticulectomy | * | 1 | |||||||||
| High risk (> 15% incidence) | Resection of anterior mediastinal mass | * | 1 | ||||||||
| Thoracoscopic lobectomy | * | 1 | |||||||||
| Open thoracotomy for lobectomy | * | 1 | |||||||||
| Tracheal resection and reconstruction/carinal resection | * | 1 | |||||||||
| Pneumonectomy | * | * | 2 | ||||||||
| Pleurectomy | * | * | 2 | ||||||||
| Volume reduction/bullectomy | * | 1 | |||||||||
| Bronchopleural fistula repair | * | 1 | |||||||||
| Clagett window | * | 1 | |||||||||
| Lung transplantation | * | * | 2 | ||||||||
| Esophagectomy | * | 1 | |||||||||
| Pericardial window | * | 1 | |||||||||
| 14 | 43 | 12 | 10 | 0 | 0 | 0 | 0 | ||||
POAF treatments: level of evidence
| Characteristics - subcomponents | STS | AATS | ACC AHA & ESC | ACS | SCAI | ACCP | HFSA | ESC | Count | ||
| All patients | Class I | Reduce or stop catecholaminergic inotropic agents | * | 1 | |||||||
| Optimize fluids and maintain normal electrolyte levels | * | 1 | |||||||||
| Evaluate/treat any possible triggering factors | * | * | 2 | ||||||||
| A non-dihydropyridine CCB is recommended when beta-blockers are inadequate in achieving rate control | * | 1 | |||||||||
| Maintain Mg > 2 mg/dL | * | 1 | |||||||||
| Maintain K > 4 mmol/L | * | 1 | |||||||||
| Treat w/ beta-blocker unless contraindicated | * | 1 | |||||||||
| Restart home beta-blocker (if applicable) | * | 1 | |||||||||
| Check TSH levels | * | 1 | |||||||||
| Class IIa | Synchronized electrical cardioversion or Ibutilide as recommended for nonsurgical pts | * | 1 | ||||||||
| Hemodynamically unstable | Class I | Synchronized electrical cardioversion within | * | 1 | |||||||
| Synchronized electrical cardioversion after 48 h and w/ anticoagulation continued for 4 weeks | * | 1 | |||||||||
| Synchronized electrical cardioversion | * | * | 2 | ||||||||
| Class IIa | If cardioversion is unsuccessful initiate rate and rhythm control w/ IV esmolol, diltiazem, digoxin, or amiodarone while preparing repeat cardioversion | * | 1 | ||||||||
| Treat recurrent or refractory POAF through antiarrhythmic medications as recommended by pts w/ CAD who develop AF | * | 1 | |||||||||
| Should initially manage w/ rate control and anticoagulation | * | 1 | |||||||||
| Class IIb | Cardiology consultation may be useful | * | 1 | ||||||||
| Hemodynamically stable | Class I | Pts w/ hemodynamically stable and symptomatically acceptable POAF should receive a rate control lasting approximately 24 h | * | 1 | |||||||
| Pts w/ hemodynamically stable but symptomatically intolerable AF should be chemically or electrically cardioverted | * | 1 | |||||||||
| Class IIa | Manage w/ rate control strategy | * | * | 2 | |||||||
| Pharmacologic or cardioversion is reasonable in pts who have recurrent or refractory POAF are uncontrolled v. rates or medication symptoms | * | 1 | |||||||||
| Pts w/ hemodynamically stable, continuous, or recurrent, POAF ongoing > 24 h after initiation of rate control, it is reasonable to attempt chemical cardioversion | * | 1 | |||||||||
| Pharmacologic or electrical cardioversion is reasonable in pts who are nearing 48 h new-onset POAF that have contraindications for anticoagulation | * | 1 | |||||||||
| Antiarrhythmic medication should be considered to restore sinus rhythm | * | * | 2 | ||||||||
| Class IIb | Pts w/ hemodynamically stable, continuous, or recurrent, POAF ongoing after chemical cardioversion may be considered for an electrical cardioversion | * | 1 | ||||||||
| IV Vernakalant may be considered for cardioversion w/o severe HF, HTN, or severe structural heart disease | * | 1 | |||||||||
| Anticoagulation | Class I | For POAF < 48 h, anticoagulation should be based on CHA2DS2-VASc risk score for the pt | * | 1 | |||||||
| For POAF > 48 h, antithrombotic medications are recommended as recommended to non-surgical pts | * | 1 | |||||||||
| Consider anticoagulation if AF > 48 h | * | 1 | |||||||||
| Administer antithrombotic medication as recommended for nonsurgical pts | * | 1 | |||||||||
| Class IIa | For pts w/ 2+ risk factors w/ POAF > 48 h, anticoagulation is reasonable if not contraindicated | * | 1 | ||||||||
| For pts w/ < 2 risk factors and not suitable for warfarin w/ PAOF > 48 h, aspirin (325 mg), is reasonable if not contraindicated | * | 1 | |||||||||
| It is reasonable to administer antithrombotic medication in pts, as advised for nonsurgical pts | * | 1 | |||||||||
| Long term anticoagulation should be considered for pts at risk for stroke | * | 1 | |||||||||
| NOACs (dabigatran, rivaroxaban, apixaban) are reasonable as an alternative to warfarin for pts w/o prosthetic heart valve, valve disease, and or renal impairment or risk of gastrointestinal bleeding | * | 1 | |||||||||
| It is reasonable to continue anticoagulation therapy for 4 weeks after the return of sinus rhythm | * | 1 | |||||||||
| Class III | NOACs should be avoided for pts at risk for serious bleeding | * | 1 | ||||||||
| In high-risk POAF (history of stroke or TIA), heparin should be considered | * | 1 | |||||||||
| Recommended to continue anticoagulation therapy 30 days after return to sinus rhythm | * | 1 | |||||||||
| Rate | Class I | IV of B-blockers or Non-dihydropyridine CCB for patients w/ rapid ventricular response | * | 1 | |||||||
| Caution should be used with pts w/ hypotension, LV dysfunction, or HF | * | 1 | |||||||||
| A selective B1-blocking agent is recommended as the initial drug for rate control in the absence of moderate-severe chronic obstructive pulmonary disease or active bronchospasm | * | 1 | |||||||||
| Diltiazem should be the first agent used in the presence of moderate-severe chronic obstructive pulmonary disease or active bronchospasm. | * | 1 | |||||||||
| Class IIa | Combo of AV nodal blocking agents: B-blockers, non-dihydropyridine CCB, or digoxin can be useful if single-agent fails | * | 1 | ||||||||
| For pts, w/ hypotension, HF, or LV dysfunction IV amiodarone can be useful | * | 1 | |||||||||
| Class IIb | For pts, w/ hypotension, HF, or LV dysfunction IV digoxin can be useful | * | 1 | ||||||||
| Class III | For pts, w/ preexcitation and POAF use of AV nodal blocking agents: beta-blockers, IV amiodarone, non-dihydropyridine CCB, or digoxin should be avoided | * | 1 | ||||||||
| Digoxin as a single agent should not be used for rate control, although it may be effective in combination with a B1-blocker or diltiazem. | * | 1 | |||||||||
| Rhythm | Class IIa | IV Amiodarone is useful for pharmacologic cardioversion of POAF | * | 1 | |||||||
| It is reasonable to restore sinus rhythm pharmacologically w/ ibutilide or cardioversion | * | 1 | |||||||||
| Amiodarone, sotalol, flecainide, propafenone, or dofetilide can be useful to maintain sinus rhythm | * | 1 | |||||||||
| When chemical cardioversion is employed in the setting of continuous or recurrent POAF, the most reasonable initial drugs are IV followed by oral amiodarone or oral flecainide | * | 1 | |||||||||
| Class IIb | Flecainide or propafenone may be considered for pharmacologic cardioversion of POAF if the pt has had no previous history of MI, CAD, LV dysfunction, LV hypertrophy, or valvular disease considered moderate or greater | * | 1 | ||||||||
| IV ibutilide or procainamide may be considered in pts w/ structural heart disease w/o hypotension or congestive HF | * | 1 | |||||||||
| IV ibutilide or procainamide may be considered for pts w/ an accessory pathway | * | 1 | |||||||||
| Class III | Amiodarone is not recommended in pts who are mechanically ventilated, who have undergone pneumonectomy, or who have substantial pre-existing lung disease | * | 1 | ||||||||
| Flecainide should not be used in pts with any history of structural cardiac disease, including ventricular hypertrophy, systolic dysfunction, or any valve or coronary disease | * | * | 2 | ||||||||
| Dronedarone should not be used for the treatment of POAF in pts w/ HF | * | 1 | |||||||||
| 13 | 29 | 9 | 6 | 0 | 2 | 0 | 5 |
RESULTS
Part I - POAF definitional components
Of the ten professional societies analyzed 50% (n = 5) did not define POAF. Table 1 presents the results of POAF definition characteristics by society. Not unexpectedly, of the 4 CT societies included 75% (n = 3) defined POAF in contrast to only 33% of non-CT societies.
The STS’s POAF definition described in [Table 1] was updated in 2014. Prior to this update, its definition was “atrial fibrillation requiring treatment”, and this was the most frequently referenced by independent manuscripts (n = 13/71; 18%).
Tables 2 and 3 classify the POAF definitional characteristics from the 51 independent manuscripts. Specific electrocardiogram characteristics were most frequently mentioned at 86% (n = 44) along with new-onset POAF (53%; n = 27). All but one publication stated that the clinical significance of a POAF episode should be less than or equal to one hour; thus, there was the most uniformity in this PAOF component. While not clearly a majority, the largest consensus among publications (n = 22/71; 31%) considered at least 30 s to be clinically significant POAF; this was a point also shared by professional societies where 2 of the 3 that noted episode duration criteria also used 30 s as their standard.
Based on this detailed review, great variability was observed across all three tables. In [Table 1] 76%
Between societies and independent manuscripts, the most variability was seen between first POAF observation timing and diversity of general definitions with only 24% (n = 8/33) of this criteria’s subcomponents in agreement.
Part II - guideline recommendations for POAF patient management
Across the ten professional societies guidelines, only eight included one or more management strategies for POAF classified based on the three listed strategies. Of these eight societies, three did not independently define postoperative atrial fibrillation but referred to another published atrial fibrillation definition. Five societies provided risk assessment guidelines [Table 6], seven societies published POAF prevention guidelines [Table 5], and all eight societies provided POAF management guidelines [Table 7].
In evaluating POAF risk, eight risk characteristics were commonly identified (> 50% consensus); all of these risk factors were viewed as non-modifiable, including preoperative atrial arrhythmias, valvular disease, congestive heart failure, pericarditis, advancing age, male gender, and chronic lung disease. Advanced age had the greatest level (75%) of consensus among societies; advanced age as a risk for POAF has been identified by the literature[14]. Three thoracic surgery procedures that drew consensus between STS and AATS and identified a high incidence of POAF (> 15%) were pneumonectomy, pleurectomy, and lung transplantation. As a modifiable risk factor, HTN was mentioned but only rarely.
Across the eight prophylactic guidelines evaluated, the greatest level of consensus was found for the use of B-blockers (n = 5 society-based guidelines) and amiodarone (n = 6 society-based guidelines). Unlike the risk assessment guidelines, 68% (n = 17/25) of the prophylactic recommendations were provided by procedural societies. Between these two procedural societies, AATS & STS, though only two were jointly recommended, “Avoid B-blocker withdrawal” and “Magnesium supplementation”.
Management guidelines were similarly reported (65%; n = 42/64) primarily by procedural societies. Agreement was seen broadly among categories used. Eight societies provided guidelines and of these, eight provided guidance for anticoagulation, six provided guidance to ensure hemodynamic stability, six provided guidance for the sub-group of hemodynamic unstable POAF patients, five for all POAF patients, five for rhythm control POAF patients, and two for rate control POAF patients. These categories once expanded upon [Table 6] showed 58 recommendations of which only five were used by more than one society (n = 5/58; 8%).
DISCUSSION
This literature review summarized the guidelines and guideline key references evaluated. The purpose of this review was to describe the current POAF landscape. Through careful examination of definitions, risks, prevention, and management among both professional societies and literature, there is considerable evidence showing the extensive heterogeneity in defining and managing this POAF condition.
Comparing the POAF definitional components, an outstanding question is how can a POAF definition be constructed optimally? Balancing definitional sensitivity and specificity is crucial. When evaluating the STS and AATS POAF definitions, it is clear that these two societies define POAF very differently.
• STS definition: “POAF is defined as atrial fibrillation over one hour or requiring treatment”.
• AATS definition: “POAF is defined as an absence of P waves and irregular RR intervals with episodes lasting at least 30 s or the length of the EKG strip (if less than 30 s). New-onset is defined as lasting < 48 h and persistent > 48 h. Symptoms usually include severe hypotension, acute myocardial ischemia, ischemia, and pulmonary edema/heart failure. Clinically significant PAOF requires rhythm control, anti-coagulation, and/or extents hospitalization[8]”.
It can be argued that AATS’s definition, which has many layers, is in comparison to STS’s definition more restrictive in nature. This pull and tug of inclusivity and restrictiveness have consequences when attempting to capture the true incidence of clinically relevant POAF.
Filardo et al.[15] provided a lens into how studies could be conducted to measure if a definition is truly capturing this data. It used the pre-2014 STS definition, “atrial fibrillation requiring treatment” and estimated that up to 3.6% of patients post-coronary artery bypass graft every year are not identified to have clinically relevant POAF[15]. This begs the question if the new STS definition improves upon this estimation and also if AATS (by approaching their definition with more “layers”) is less inclusive.
In addition to correctly estimating the incidence of clinically relevant POAF, a universal definition will be critically important to facilitate future POAF research. Without POAF definitional consensus, researchers are not able to compare different POAF-related study conclusions as to the impact of POAF on subsequent morbidity, mortality, and cost. Furthermore, it will be challenging to compare the cost-effectiveness of POAF patient management[15].
It is of great importance to place this responsibility on the correct groups. Will independent researchers come up with the needed clinical evidence to create such a universal definition or should professional societies take the mantle? Within professional societies, it is also important to note the gap of potential priorities for CT societies vs. non-CT societies. Earlier we noted a large discrepancy where 75% of CT societies vs. 33% of non-CT societies defined POAF. This could highlight potential roadblocks to which society might be better positioned to provide the scientific community with a proper universal POAF definition.
Currently, among most literature, advanced age is nearly universally an agreed upon POAF risk factor; yet
The aggregation of most current prevention and management guidelines into [Tables 5-7] is to serve as an aid for physicians and future studies. Areas of consensus show where future clinical trials could focus their attention such as the prophylactic role of B-blocker and amiodarone use. Management guidelines show more variability than prevention guidelines with only 8% of recommendations advocated by more than one society.
Such a disparity correlates with the current landscape of POAF. Not only is the occurrence of POAF as high as 50% in cardiac procedures, but its recurrence once treated is over 50% over a two-year period[1,2,16]. This shows that a proven system for treatment and prevention has not been achieved. It would be of value if a study could show the incidence rate over time of POAF and its correlation to new management/prevention guidelines.
Many other contributing factors should be considered when looking at such a high incidence rate of POAF. One of which is a serious lack of high-quality, randomized controlled trials[16]. This could stem from a refusal of acknowledgment or visibility among professional societies. For example, among the medical societies, the 2020 update to the ESC guidelines for atrial fibrillation mentions POAF in only 2 of its 126 pages, and the updated 2014 AHA/ACC/HRS guidelines for atrial fibrillation mention POAF in only 2 of its 76 pages. Among the procedural societies, STS and AATS, there has not been an update to POAF guidelines for 9 and 6 years, respectively.
The variability among definitions also creates large challenges when comparing different clinical studies. One manuscript might consider POAF lasting > 30 s, while another more restrictive study could propose to look at POAF lasting > 5 min. Regardless of the specific variability, this diversity in POAF definitions hampers meta-studies that could evaluate treatment options.
Based on the results found on POAF variability, we propose the following loose definition to be used as a placeholder until future evidence-based definitions are discovered. This definition is based on consensus from independent publications and professional societies: new-onset AF should be defined based on ECG findings longer than 30 s. Treatment or symptoms are confirmatory but do not provide adequate evidence of clinical new-onset AF.
It is also crucial to arrive at such a conclusion to use our current surgical databases to their highest potential. Currently, STS has the world’s gold standard clinical outcomes registry in adult cardiac surgery. Since its inception, more than 100 publications have utilized its information, and it currently contains more than
At this time, AATS is creating a new cardiac surgery database which may likely soon achieve the same STS level of importance to the scientific community[18]. This highlights how crucial it is that the data physicians’ daily input be of the highest quality and the greatest consistency. As the scientific community works to find the true impact that POAF has on patients, it must use data that is consistent and based upon clinical significance.
In summary, POAF has not been consistently defined by all professional societies as an important post-procedural complication. Instead of being classified uniformly as major morbidity, POAF is frequently considered a surgical nuisance; however, it should be viewed as a serious morbid complication that can lead to stroke and other emboli complications as well as congestive heart failure. Building upon Filardo’s initial study, therefore, additional POAF research now appears warranted. In order to optimize the future effectiveness and efficiency of cardiac surgical care, a clinically relevant POAF definition needs to be established[15]. Moreover, high-quality, randomized, controlled clinical trials are needed to evaluate the current POAF prevention and management strategies. Although atrial fibrillation medication-based trials have been completed, the lack of visibility and urgency towards finding options to address new-onset POAF has stalled. Hopefully, this review highlights the significance of POAF to future cardiac surgical quality improvement efforts, building an urgency to establish a POAF definitional consensus to reduce the prevalence and burden of this important condition.
DECLARATIONS
Authors’ contributionsMade substantial contributions to this study’s conceptualization and qualitative design: Pardo D, Rove JY, Grover FL, Shroyer AL
Coordinated the literature review, captured the study data, performed the preliminary analysis, and provided summary reports describing this study’s findings: Pardo D
Verified a sampling of the data captured and guided the analyses performed: Shroyer AL
Assisted with data report interpretation: Rove JY, Grover FL
Prepared the first manuscript draft: Pardo D, Shroyer AL
Revised the manuscript substantively and provided final manuscript approval: Pardo D, Rove JY,
Not applicable.
Financial support and sponsorshipNone
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Hindricks G, Potpara T, Dagres N, et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373-498.
2. Hogue CW Jr, Creswell LL, Gutterman DD, Fleisher LA. American College of Chest Physicians. Epidemiology, mechanisms, and risks: American College of Chest Physicians guidelines for the prevention and management of postoperative atrial fibrillation after cardiac surgery. Chest 2005;128:9S-16S.
3. Dobrev D, Aguilar M, Heijman J, Guichard JB, Nattel S. Postoperative atrial fibrillation: mechanisms, manifestations and management. Nat Rev Cardiol 2019;16:417-36.
4. Marjoua Y, Bozic KJ. Brief history of quality movement in US healthcare. Curr Rev Musculoskelet Med 2012;5:265-73.
5. Shroyer AL, London MJ, VillaNueva CB, et al. The processes, structures, and outcomes of care in cardiac surgery study protocol. Med Care 1995;33:OS17-25.
6. Adult Cardiac Surgery Database Data Collection. Available from: https://www.sts.org/registries-research-center/sts-national-database/adult-cardiac-surgery-database/data-collection [Last accessed on 25 Jan 2022].
7. Khuri SF, Daley J, Henderson W, et al. The Department of Veterans Affairs’ NSQIP: the first national, validated, outcome-based, risk-adjusted, and peer-controlled program for the measurement and enhancement of the quality of surgical care. National VA Surgical Quality Improvement Program. Ann Surg 1998;228:491-507.
8. Frendl G, Sodickson AC, Chung MK, et al. American Association for Thoracic Surgery. 2014 AATS guidelines for the prevention and management of perioperative atrial fibrillation and flutter for thoracic surgical procedures. J Thorac Cardiovasc Surg 2014;148:e153-93.
9. Atrial Fibrillation & Stroke. Available from: http://www.secondscount.org/heart-condition-centers/info-detail-2/atrial-fibrillation-stroke [Last accessed on 25 Jan 2022].
10. Danelich IM, Lose JM, Wright SS, et al. Practical management of postoperative atrial fibrillation after noncardiac surgery. J Am Coll Surg 2014;219:831-41.
11. January CT, Wann LS, Alpert JS, et al. ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014;130:e199-267.
12. Calkins H, Hindricks G, Cappato R, et al. Document Reviewers. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018;20:e1-160.
13. Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018;154:1121-201.
14. Burrage PS, Low YH, Campbell NG, O’Brien B. New-onset atrial fibrillation in adult patients after cardiac surgery. Curr Anesthesiol Rep 2019;9:174-93.
15. Filardo G, Pollock BD, da Graca B, et al. Underestimation of the incidence of new-onset post-coronary artery bypass grafting atrial fibrillation and its impact on 30-day mortality. J Thorac Cardiovasc Surg 2017;154:1260-6.
16. Riad FS, German K, Deitz S, Sahadevan J, Sundaram V, Waldo AL. Attitudes toward anticoagulation for postoperative atrial fibrillation: a nationwide survey of VA providers. Pacing Clin Electrophysiol 2020;43:1295-301.
17. Adult Cardiac Surgery Database. Available from: https://www.sts.org/registries/sts-national-database/adult-cardiac-surgery-database [Last accessed on 25 Jan 2022].
18. Blackstone EH, Swain J, McCardle K, Adams DH. Governance Committee, American Association for Thoracic Surgery Quality Assessment Program. A comprehensive American Association for Thoracic Surgery quality program for the 21st century. J Thorac Cardiovasc Surg 2019;158:1120-6.
19. Therrien J, Siu SC, Harris L, et al. Impact of pulmonary valve replacement on arrhythmia propensity late after repair of tetralogy of Fallot. Circulation 2001;103:2489-94.
20. Amar D, Shi W, Hogue CW Jr, et al. Clinical prediction rule for atrial fibrillation after coronary artery bypass grafting. J Am Coll Cardiol 2004;44:1248-53.
21. White CM, Kluger J, Lertsburapa K, Faheem O, Coleman CI. Effect of preoperative angiotensin converting enzyme inhibitor or angiotensin receptor blocker use on the frequency of atrial fibrillation after cardiac surgery: a cohort study from the atrial fibrillation suppression trials II and III. Eur J Cardiothorac Surg 2007;31:817-20.
22. Echahidi N, Mohty D, Pibarot P, et al. Obesity and metabolic syndrome are independent risk factors for atrial fibrillation after coronary artery bypass graft surgery. Circulation 2007;116:I213-9.
23. Roshanali F, Mandegar MH, Yousefnia MA, Rayatzadeh H, Alaeddini F, Amouzadeh F. Prediction of atrial fibrillation via atrial electromechanical interval after coronary artery bypass grafting. Circulation 2007;116:2012-7.
24. Goette A, Lendeckel U, Kuchenbecker A, et al. Cigarette smoking induces atrial fibrosis in humans via nicotine. Heart 2007;93:1056-63.
25. Ahlsson AJ, Bodin L, Lundblad OH, Englund AG. Postoperative atrial fibrillation is not correlated to C-reactive protein. Ann Thorac Surg 2007;83:1332-7.
26. Spies C, Khandelwal A, Timmermanns I, Schräder R. Incidence of atrial fibrillation following transcatheter closure of atrial septal defects in adults. Am J Cardiol 2008;102:902-6.
27. Serafimovski N, Burke P, Khawaja O, Sekulic M, Machado C. Usefulness of dofetilide for the prevention of atrial tachyarrhythmias (atrial fibrillation or flutter) after coronary artery bypass grafting. Am J Cardiol 2008;101:1574-9.
28. Braga S, Vaninetti R, Pedretti RF. Plasma B-type natriuretic peptide predicts atrial fibrillation during rehabilitation after cardiac surgery. Eur J Cardiovasc Prev Rehabil 2008;15:460-6.
29. Afzal AR, Mandal K, Nyamweya S, et al. Association of Met439Thr substitution in heat shock protein 70 gene with postoperative atrial fibrillation and serum HSP70 protein levels. Cardiology 2008;110:45-52.
30. Roshanali F, Mandegar MH, Yousefnia MA, Alaeddini F, Saidi B. Prevention of atrial fibrillation after coronary artery bypass grafting via atrial electromechanical interval and use of amiodarone prophylaxis. Interact Cardiovasc Thorac Surg 2009;8:421-5.
31. Mariscalco G, Sarzi Braga S, Banach M, et al. Preoperative n-3 polyunsatured fatty acids are associated with a decrease in the incidence of early atrial fibrillation following cardiac surgery. Angiology 2010;61:643-50.
32. Heidarsdottir R, Arnar DO, Skuladottir GV, et al. Does treatment with n-3 polyunsaturated fatty acids prevent atrial fibrillation after open heart surgery? Europace 2010;12:356-63.
33. Skuladottir GV, Heidarsdottir R, Arnar DO, et al. Plasma n-3 and n-6 fatty acids and the incidence of atrial fibrillation following coronary artery bypass graft surgery. Eur J Clin Invest 2011;41:995-1003.
34. Veasey RA, Segal OR, Large JK, et al. The efficacy of intraoperative atrial radiofrequency ablation for atrial fibrillation during concomitant cardiac surgery-the Surgical Atrial Fibrillation Suppression (SAFS) Study. J Interv Card Electrophysiol 2011;32:29-35.
35. Melduni RM, Suri RM, Seward JB, et al. Diastolic dysfunction in patients undergoing cardiac surgery: a pathophysiological mechanism underlying the initiation of new-onset post-operative atrial fibrillation. J Am Coll Cardiol 2011;58:953-61.
36. Nuis RJ, Van Mieghem NM, Schultz CJ, et al. Frequency and causes of stroke during or after transcatheter aortic valve implantation. Am J Cardiol 2012;109:1637-43.
37. Bolesta S, Aungst TD, Kong F. Effect of sodium nitroprusside on the occurrence of atrial fibrillation after cardiothoracic surgery. Ann Pharmacother 2012;46:785-92.
38. Amat-Santos IJ, Rodés-Cabau J, Urena M, et al. Incidence, predictive factors, and prognostic value of new-onset atrial fibrillation following transcatheter aortic valve implantation. J Am Coll Cardiol 2012;59:178-88.
39. Cao H, Zhou Q, Wu Y, et al. Preoperative serum soluble receptor activator of nuclear factor-κB ligand and osteoprotegerin predict postoperative atrial fibrillation in patients undergoing cardiac valve surgery. Ann Thorac Surg 2013;96:800-6.
40. Chua S, Shyu K, Lu M, et al. Association between renal function, diastolic dysfunction, and postoperative atrial fibrillation following cardiac surgery. Circ J 2013;77:2303-10.
41. Kallel S, Jarrya A, Triki Z, Abdenadher M, Frikha J, Karoui A. The use of N-terminal pro-brain natriuretic peptide as a predictor of atrial fibrillation after cardiac surgery. J Cardiovasc Surg (Torino) 2013;54:403-11.
42. Pecha S, Schäfer T, Subbotina I, Ahmadzade T, Reichenspurner H, Wagner FM. Rhythm outcome predictors after concomitant surgical ablation for atrial fibrillation: a 9-year, single-center experience. J Thorac Cardiovasc Surg 2014;148:428-33.
43. Yankelson L, Steinvil A, Gershovitz L, et al. Atrial fibrillation, stroke, and mortality rates after transcatheter aortic valve implantation. Am J Cardiol 2014;114:1861-6.
44. Wong JK, Lobato RL, Pinesett A, Maxwell BG, Mora-Mangano CT, Perez MV. P-wave characteristics on routine preoperative electrocardiogram improve prediction of new-onset postoperative atrial fibrillation in cardiac surgery. J Cardiothorac Vasc Anesth 2014;28:1497-504.
45. Metcalf RG, Skuladottir GV, Indridason OS, et al. U-shaped relationship between tissue docosahexaenoic acid and atrial fibrillation following cardiac surgery. Eur J Clin Nutr 2014;68:114-8.
46. Imanishi J, Tanaka H, Sawa T, et al. Left atrial booster-pump function as a predictive parameter for new-onset postoperative atrial fibrillation in patients with severe aortic stenosis. Int J Cardiovasc Imaging 2014;30:295-304.
47. van Osch D, Dieleman JM, van Dijk D, et al. DExamethasone for Cardiac Surgery (DECS) study group, DExamethasone for Cardiac Surgery DECS study group. Dexamethasone for the prevention of postoperative atrial fibrillation. Int J Cardiol 2015;182:431-7.
48. Patti G, Bennett R, Seshasai SR, et al. Statin pretreatment and risk of in-hospital atrial fibrillation among patients undergoing cardiac surgery: a collaborative meta-analysis of 11 randomized controlled trials. Europace 2015;17:855-63.
49. Guenancia C, Pujos C, Debomy F, Malapert G, Laurent G, Bouchot O. Incidence and predictors of new-onset silent atrial fibrillation after coronary artery bypass graft surgery. Biomed Res Int 2015;2015:703685.
50. Chua SK, Shyu KG, Lu MJ, et al. Renal dysfunction and the risk of postoperative atrial fibrillation after cardiac surgery: role beyond the CHA2DS2-VASc score. Europace 2015;17:1363-70.
51. Bouchot O, Guenancia C, Kahli A, et al. Low circulating levels of growth differentiation factor-15 before coronary artery bypass surgery may predict postoperative atrial fibrillation. J Cardiothorac Vasc Anesth 2015;29:1131-9.
52. Wong JK, Maxwell BG, Kushida CA, et al. Obstructive sleep apnea is an independent predictor of postoperative atrial fibrillation in cardiac surgery. J Cardiothorac Vasc Anesth 2015;29:1140-7.
53. Magruder JT, Plum W, Crawford TC, et al. Incidence of late atrial fibrillation in bilateral lung versus heart transplants. Asian Cardiovasc Thorac Ann 2016;24:772-8.
54. Tarantini G, Mojoli M, Windecker S, et al. Prevalence and impact of atrial fibrillation in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement: an analysis from the SOURCE XT prospective multicenter registry. JACC Cardiovasc Interv 2016;9:937-46.
55. El-Chami MF, Merchant FM, Smith P, et al. Management of new-onset postoperative atrial fibrillation utilizing insertable cardiac monitor technology to observe recurrence of AF (MONITOR-AF). Pacing Clin Electrophysiol 2016;39:1083-9.
56. Zhang W, Liu W, Chew ST, Shen L, Ti LK. A clinical prediction model for postcardiac surgery atrial fibrillation in an asian population. Anesth Analg 2016;123:283-9.
57. Moscarelli M, Cerillo A, Athanasiou T, et al. Minimally invasive mitral valve surgery in high-risk patients: operating outside the boxplot. Interact Cardiovasc Thorac Surg 2016;22:756-61.
58. Furuta A, Lellouche N, Mouillet G, et al. Prognostic value of new onset atrial fibrillation after transcatheter aortic valve implantation: a FRANCE 2 registry substudy. Int J Cardiol 2016;210:72-9.
59. Magruder JT, Collica S, Belmustakov S, et al. Predictors of late-onset atrial fibrillation following isolated mitral valve repairs in patients with preserved ejection fraction. J Card Surg 2016;31:486-92.
60. Ting PC, Chou AH, Chien-Chia Wu V, et al. Relationship between right ventricular function and atrial fibrillation after cardiac surgery. J Cardiothorac Vasc Anesth 2017;31:1663-71.
61. Cerit L, Kemal H, Gulsen K, Ozcem B, Cerit Z, Duygu H. Relationship between Vitamin D and the development of atrial fibrillation after on-pump coronary artery bypass graft surgery. Cardiovasc J Afr 2017;28:104-7.
62. Vasheghani Farahani A, Yousefi Azar A, Goodarzynejad HR, et al. Fish oil supplementation for primary prevention of atrial fibrillation after coronary artery bypass graft surgery: a randomized clinical trial. Int J Surg 2017;42:41-8.
63. Harling L, Lambert J, Ashrafian H, Darzi A, Gooderham NJ, Athanasiou T. Elevated serum microRNA 483-5p levels may predict patients at risk of post-operative atrial fibrillation. Eur J Cardiothorac Surg 2017;51:73-8.
64. Harling L, Lambert J, Ashrafian H, Darzi A, Gooderham NJ, Athanasiou T. Pre-operative serum VCAM-1 as a biomarker of atrial fibrillation after coronary artery bypass grafting. J Cardiothorac Surg 2017;12:70.
65. Wong JK, Mariano ER, Doufas AG, Olejniczak MJ, Kushida CA. Preoperative treatment of obstructive sleep apnea with positive airway pressure is associated with decreased incidence of atrial fibrillation after cardiac surgery. J Cardiothorac Vasc Anesth 2017;31:1250-6.
66. Robert R, Porot G, Vernay C, et al. Incidence, predictive factors, and prognostic impact of silent atrial fibrillation after transcatheter aortic valve implantation. Am J Cardiol 2018;122:446-54.
67. Magne J, Salerno B, Mohty D, et al. Echocardiography is useful to predict postoperative atrial fibrillation in patients undergoing isolated coronary bypass surgery: a prospective study. Eur Heart J Acute Cardiovasc Care 2019;8:104-13.
68. Mentias A, Saad M, Girotra S, et al. Impact of pre-existing and new-onset atrial fibrillation on outcomes after transcatheter aortic valve replacement. JACC Cardiovasc Interv 2019;12:2119-29.
69. Atreya AR, Priya A, Pack QR, et al. Use and outcomes associated with perioperative amiodarone in cardiac surgery. J Am Heart Assoc 2019;8:e009892.
70. Corradi D, Saffitz JE, Novelli D, et al. Prospective evaluation of clinico-pathological predictors of postoperative atrial fibrillation: an ancillary study from the OPERA trial. Circ Arrhythm Electrophysiol 2020;13:e008382.
71. Mendes LA, Connelly GP, Mckenney PA, et al. Right coronary artery stenosis: an independent predictor of atrial fibrillation after coronary artery bypass surgery. J Am Coll Cardiol 1995;25:198-202.
72. Solomon AJ, Greenberg MD, Kilborn MJ, Katz NM. Amiodarone versus a beta-blocker to prevent atrial fibrillation after cardiovascular surgery. Am Heart J 2001;142:811-5.
73. Hogue CW Jr, Palin CA, Kailasam R, et al. C-reactive protein levels and atrial fibrillation after cardiac surgery in women. Ann Thorac Surg 2006;82:97-102.
74. Ozin B, Sezgin A, Atar I, et al. Effectiveness of triple-site triggered atrial pacing for prevention of atrial fibrillation after coronary artery bypass graft surgery. Clin Cardiol 2005;28:479-82.
75. Dogan SM, Buyukates M, Kandemir O, et al. Predictors of atrial fibrillation after coronary artery bypass surgery. Coron Artery Dis 2007;18:327-31.
76. Tsuboi J, Kawazoe K, Izumoto H, Okabayashi H. Postoperative treatment with carvedilol, a beta-adrenergic blocker, prevents paroxysmal atrial fibrillation after coronary artery bypass grafting. Circ J 2008;72:588-91.
77. Ito N, Tashiro T, Morishige N, et al. Efficacy of propafenone hydrochloride in preventing postoperative atrial fibrillation after coronary artery bypass grafting. Heart Surg Forum 2010;13:E223-7.
78. Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy a meta-analysis of randomized trials. J Am Coll Cardiol 2010;56:1099-109.
79. Kaw R, Hernandez AV, Masood I, Gillinov AM, Saliba W, Blackstone EH. Short- and long-term mortality associated with new-onset atrial fibrillation after coronary artery bypass grafting: a systematic review and meta-analysis. J Thorac Cardiovasc Surg 2011;141:1305-12.
80. Karimi A, Bidhendi LM, Rezvanfard M, et al. The effect of a high dose of atorvastatin on the occurrence of atrial fibrillation after coronary artery bypass grafting. Ann Thorac Surg 2012;94:8-14.
81. Tchetche D, Farah B, Misuraca L, et al. Cerebrovascular events post-transcatheter aortic valve replacement in a large cohort of patients: a FRANCE-2 registry substudy. JACC Cardiovasc Interv 2014;7:1138-45.
82. Ramdjan TTTK, Mouws EMJP, Teuwen CP, et al. Progression of late postoperative atrial fibrillation in patients with tetralogy of Fallot. J Cardiovasc Electrophysiol 2018;29:30-7.
83. Wadia SK, Lluri G, Aboulhosn JA, et al. Postoperative and short-term atrial tachyarrhythmia burdens after transcatheter vs surgical pulmonary valve replacement among congenital heart disease patients. Congenit Heart Dis 2019;14:838-45.
84. Serban C, Arinze JT, Starreveld R, et al. The impact of obesity on early postoperative atrial fibrillation burden. J Thorac Cardiovasc Surg 2020;159:930-8.e2.
85. Chapin TW, Leedahl DD, Brown AB, et al. Comparison of anticoagulants for postoperative atrial fibrillation after coronary artery bypass grafting: a pilot study. J Cardiovasc Pharmacol Ther 2020;25:523-30.
86. Aksoy F, Uysal D, Ibrişim E. Relationship between c-reactive protein/albumin ratio and new-onset atrial fibrillation after coronary artery bypass grafting. Rev Assoc Med Bras (1992) 2020;66:1070-6.
87. Kuyumcu MS, Uysal D, Özbay MB, Aydın O, İbrişim E. Frontal plane QRS-T angle may be a predictor for post-coronary artery bypass graft surgery atrial fibrillation. Rev Assoc Med Bras (1992) 2020;66:1673-8.
88. Aksoy F, Uysal D, Ibrişim E. Predictive values of C-reactive protein/albumin ratio in new-onset atrial fibrillation after coronary artery bypass grafting. Rev Assoc Med Bras (1992) 2020;66:1049-56.
89. Murphy GJ, Ascione R, Caputo M, Angelini GD. Operative factors that contribute to post-operative atrial fibrillation: insights from a prospective randomized trial. Card Electrophysiol Rev 2003;7:136-9.
90. Fernando HC, Jaklitsch MT, Walsh GL, et al. The Society of Thoracic Surgeons practice guideline on the prophylaxis and management of atrial fibrillation associated with general thoracic surgery: executive summary. Ann Thorac Surg 2011;92:1144-52.
91. Fuster V, Rydén LE, Cannom DS, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines, European Society of Cardiology Committee for Practice Guidelines, European Heart Rhythm Association, Heart Rhythm Society. ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006;114:e257-354.
92. Epstein AE, Alexander JC, Gutterman DD, Maisel W, Wharton JM. American College of Chest Physicians. Anticoagulation: American College of Chest Physicians guidelines for the prevention and management of postoperative atrial fibrillation after cardiac surgery. Chest 2005;128:24S-7S.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Pardo D, Grover FL, Rove JY, Shroyer ALW. Improving future postoperative atrial fibrillation care: a 30,000-foot viewpoint. Vessel Plus 2022;6:36. http://dx.doi.org/10.20517/2574-1209.2021.120
AMA Style
Pardo D, Grover FL, Rove JY, Shroyer ALW. Improving future postoperative atrial fibrillation care: a 30,000-foot viewpoint. Vessel Plus. 2022; 6: 36. http://dx.doi.org/10.20517/2574-1209.2021.120
Chicago/Turabian Style
Pardo, Daniel, Frederick L. Grover, Jessica Y. Rove, A. Laurie W. Shroyer. 2022. "Improving future postoperative atrial fibrillation care: a 30,000-foot viewpoint" Vessel Plus. 6: 36. http://dx.doi.org/10.20517/2574-1209.2021.120
ACS Style
Pardo, D.; Grover FL.; Rove JY.; Shroyer ALW. Improving future postoperative atrial fibrillation care: a 30,000-foot viewpoint. Vessel Plus. 2022, 6, 36. http://dx.doi.org/10.20517/2574-1209.2021.120
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 16 clicks
Cite This Article 16 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.